
Cardiology — MCQs

On this page
A 55-year-old man presents to his physician complaining of pain. He states that in the morning he feels rather stiff and has general discomfort and pain in his muscles. The patient has a past medical history of diabetes and is not currently taking any medications. His temperature is 99.2°F (37.3°C), blood pressure is 147/98 mmHg, pulse is 80/min, respirations are 12/min, and oxygen saturation is 99% on room air. Physical exam demonstrates mild tenderness of the patient's musculature diffusely. The patient has 2+ reflexes and 5/5 strength in his upper and lower extremities. Laboratory values are notable for an elevated erythrocyte sedimentation rate. Which of the following is the best next step in management?
A 26-year-old African-American woman comes to the physician because of a 4-day history of a nonproductive cough and chest pain. The pain is sharp and worse when she breathes deeply. During this time, she has also had two episodes of hematuria. Over the past 6 months, she has had intermittent pain, stiffness, and swelling in her fingers and left knee. She had two miscarriages at age 22 and 24. Her only medication is minocycline for acne vulgaris. Her temperature is 38.1°C (100.6°F), pulse is 75/min, and blood pressure is 138/85 mm Hg. Physical examination shows an erythematous rash on her face. There is mild tenderness over the metacarpophalangeal joints bilaterally with no warmth or erythema. Further evaluation of this patient is most likely to show which of the following findings?
A 20-year-old man is brought to the emergency department because of fever and lethargy for the past 2 days. He reports that during this time he has had occasional palpitations and shortness of breath. He has asthma and sickle cell disease. Current medications include inhaled albuterol, hydroxyurea, and folic acid. He appears fatigued. His temperature is 38.4°C (101.1°F), pulse is 122/min, respirations are 25/min, and blood pressure is 110/72 mm Hg. Examination shows pale conjunctivae. Cardiac examination shows a midsystolic ejection murmur. Laboratory studies show: Hemoglobin 6.5 g/dl Leukocyte count 5,000/mm3 Platelet count 165,000/mm3 Mean corpuscular volume 82 μm3 Reticulocyte count 0.2% Which of the following is the most likely cause of these findings?
A 51-year-old woman comes to the physician because of a 1-year history of occasional discoloration and tingling in her fingers. She has no history of major medical illness and takes no medications. Examination of the hands and fingers shows thickened, waxy skin and several firm white nodules on the fingertips. Further evaluation of this patient is most likely to show which of the following findings?
A 72-year-old woman comes to the emergency department 4 hours after the sudden onset of a diffuse, dull, throbbing headache. During this time, she also reports blurred vision, nausea, and one episode of vomiting. She has a history of hypertension and type 2 diabetes mellitus. Her medications include hydrochlorothiazide, lisinopril, atorvastatin, and metformin. She has smoked 1 pack of cigarettes daily for the past 30 years and drinks 1–2 glasses of wine per day. Her temperature is 36.6 °C (97.9 °F), pulse is 90/min, respirations are 14/min, and blood pressure is 185/110 mm Hg. Fundoscopic examination shows bilateral blurring of the optic disc margins. Physical and neurologic examinations show no other abnormalities. A complete blood count and serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference range. Urinalysis shows 2+ protein but no WBCs or RBCs. Which of the following is the most likely diagnosis?
A 56-year-old man comes to the physician for a follow-up examination. Physical examination shows hyperpigmented plaques on the posterior neck and in the axillae. His hemoglobin A1c concentration is 7.4% and fasting serum glucose concentration is 174 mg/dL. Which of the following is the strongest predisposing factor for this patient's laboratory findings?
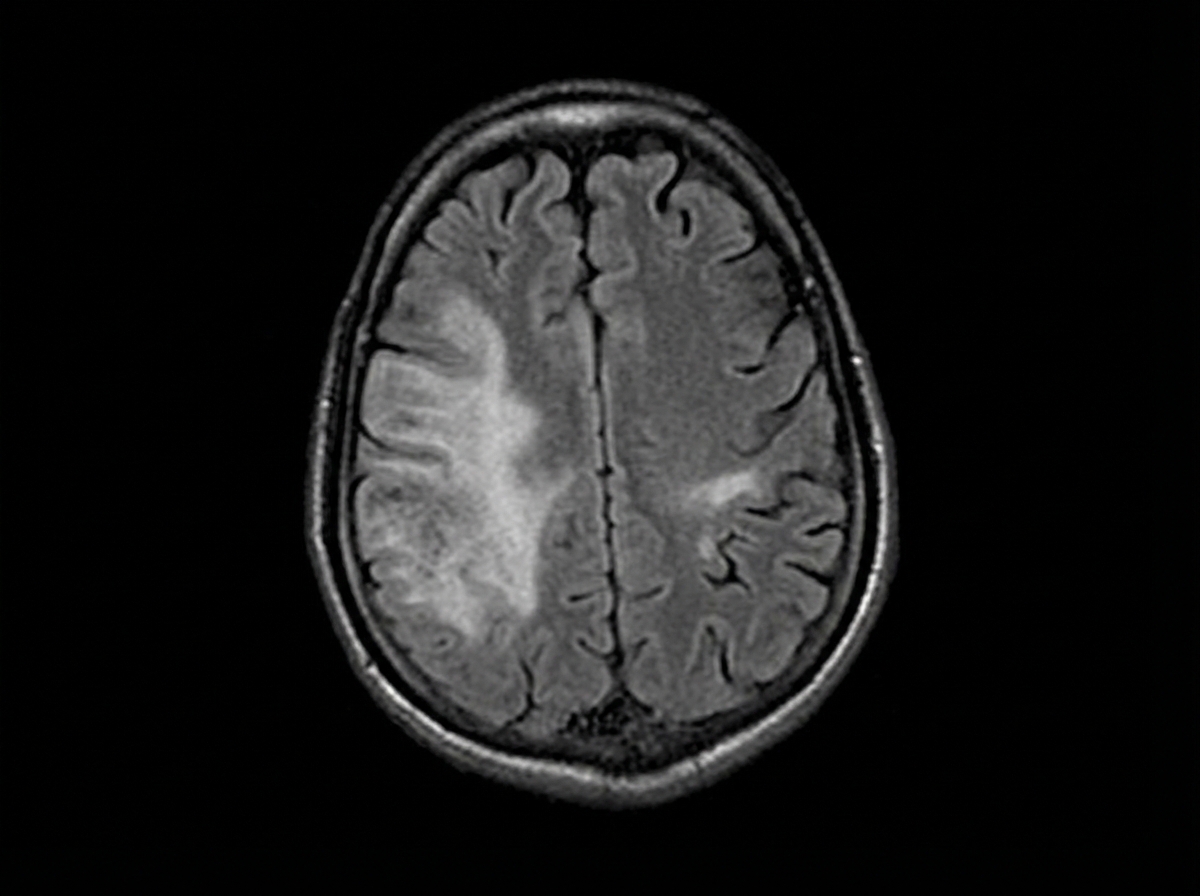
A 44-year-old man is brought to the emergency department by his daughter for a 1-week history of right leg weakness, unsteady gait, and multiple falls. During the past 6 months, he has become more forgetful and has sometimes lost his way along familiar routes. He has been having difficulties operating simple kitchen appliances such as the dishwasher and coffee maker. He has recently become increasingly paranoid, agitated, and restless. He has HIV, hypertension, and type 2 diabetes mellitus. His last visit to a physician was more than 2 years ago, and he has been noncompliant with his medications. His temperature is 37.2°C (99.0°F), blood pressure is 152/68 mm Hg, pulse is 98/min, and respiratory rate is 14/min. He is somnolent and slightly confused. He is oriented to person, but not place or time. There is mild lymphadenopathy in the cervical, axillary, and inguinal areas. Neurological examination shows right lower extremity weakness with normal tone and no other focal deficits. Laboratory studies show: Hemoglobin 9.2 g/dL Leukocyte count 3,600/mm3 Platelet count 140,000/mm3 CD4+ count 56/µL HIV viral load > 100,000 copies/mL Serum Cryptococcal antigen Negative Toxplasma gondii IgG Positive An MRI of the brain is shown below. Which of the following is the most likely diagnosis?
A previously healthy 42-year-old man is brought to the emergency department 1 hour after he was involved in a motor vehicle collision. He is conscious. He smoked one pack of cigarettes daily for 16 years but quit 8 years ago. Physical examination shows several ecchymoses over the trunk and abdomen. The abdomen is soft, and there is tenderness to palpation of the right upper quadrant without guarding or rebound. Vital signs are within normal limits. An x-ray of the chest shows no fractures; a 10-mm solid pulmonary nodule is present in the central portion of the right upper lung field. No previous x-rays of the patient are available. A CT scan of the chest is performed, which shows that the nodule has irregular, scalloped borders. Which of the following is the most appropriate next step in the management of this patient's pulmonary nodule?
A 60-year-old man comes to the physician for a routine health maintenance examination. He feels well. Five years ago, he underwent a colonoscopy, which was unremarkable. He has no history of serious illness except for an episode of poststreptococcal glomerulonephritis at the age of 10 years. His father died of bladder carcinoma at the age of 55 years. The patient works at a rubber factory. He has smoked one pack of cigarettes daily for the past 25 years. He drinks 1–2 cans of beer per day. He takes no medications. He has never received any pneumococcal vaccination. His temperature is 37°C (98.6°F), pulse is 70/min, and blood pressure is 120/80 mm Hg. Digital rectal examination shows mild symmetrical enlargement of the prostate with no masses. Which of the following is the most appropriate next step in management?
A 45-year-old woman comes to the physician because of fatigue, lightheadedness, dizziness upon standing, abdominal pain, and muscle pain over the past 6 months. She has also had an unintended weight loss of 5.8 kg (12.8 lb) over the past 3 years. She has had a history of hypoparathyroidism since she was a teenager. Her current medications include calcitriol and calcium carbonate. Her pulse is 85/min and blood pressure is 81/45 mm Hg. Physical examination shows tanned skin, as well as sparse axillary and pubic hair. Which of the following is the most likely cause of this patient's symptoms?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app