
Cardiology — MCQs

On this page
A 49-year-old man comes to the physician because of increasing difficulty achieving an erection for 6 months. During this period, he has had to reduce his hours as a construction worker because of pain in his lower back and thighs and a progressive lower limb weakness when walking for longer distances. His pain resolves after resting for a few minutes, but it recurs when he returns to work. He also reports that his pain is improved by standing still. He is sexually active with 4 female partners and uses condoms irregularly. His father has coronary artery disease and his mother died of a ruptured intracranial aneurysm at the age of 53 years. He has smoked one pack of cigarettes daily for 35 years. He has recently taken sildenafil, given to him by a friend, with no improvement in his symptoms. His only other medication is ibuprofen as needed for back pain. His last visit to a physician was 25 years ago. He is 172.5 cm (5 ft 8 in) tall and weighs 102 kg (225 lb); BMI is 34.2 kg/m2. His temperature is 36.9°C (98.4°F), pulse is 76/min, and blood pressure is 169/98 mm Hg. A complete blood count and serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference ranges. His hemoglobin A1c is 6.2%. Which of the following is the most likely finding on physical examination?
A 68-year-old man comes to the physician in July for a routine health maintenance examination. He is a retired teacher and lives in a retirement community. He has hypercholesterolemia, hypertension, and osteoarthritis of the left knee. Last year, he was diagnosed with chronic lymphocytic leukemia. A colonoscopy 8 years ago was normal. The patient had a normal digital examination and a normal prostate specific antigen level 8 months ago. The patient has never smoked and does not drink alcohol. Current medications include aspirin, lisinopril, simvastatin, chlorambucil, rituximab, and a multivitamin. His last immunizations were at a health maintenance examination 7 years ago. His temperature is 37°C (98.6°F), pulse is 82/min, respirations are 14/min, and blood pressure is 133/85 mm Hg. Examination shows a grade 2/6 systolic ejection murmur along the upper right sternal border and painless cervical lymphadenopathy. Which of the following health maintenance recommendations is most appropriate at this visit?
A 16-year-old boy comes to the physician for a routine health maintenance examination. He feels well. He has no history of serious illness. He is at the 60th percentile for height and weight. Vital signs are within normal limits. The lungs are clear to auscultation. A grade 3/6 ejection systolic murmur is heard along the lower left sternal border. The murmur decreases in intensity on rapid squatting and increases in intensity when he performs the Valsalva maneuver. This patient is at increased risk for which of the following complications?
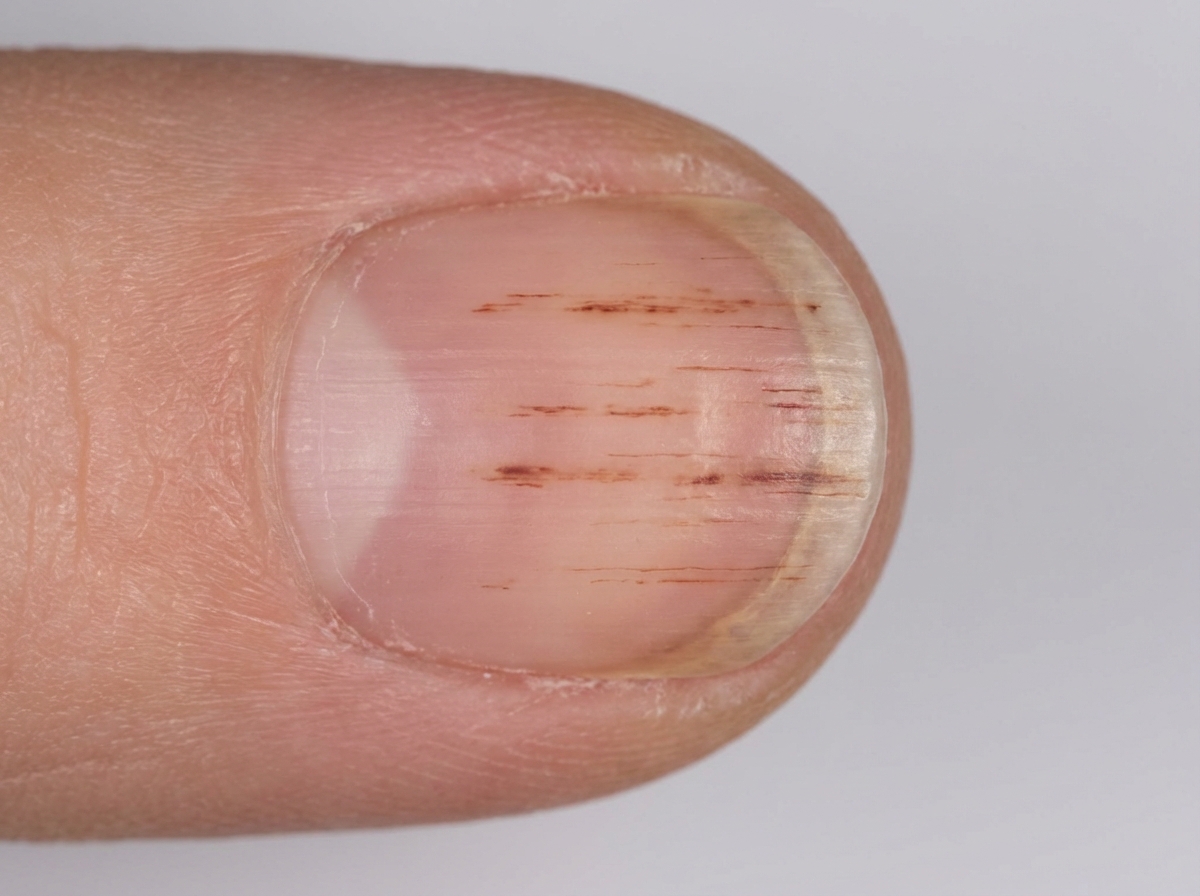
A 62-year-old man comes to the physician for a 1-month history of fever, malaise, and skin rash. He has had a 5-kg (11-lb) weight loss during this period. He does not smoke, drink alcohol, or use illicit drugs. He appears pale. His temperature is 39.1°C (102.3°F), pulse is 110/min, and blood pressure is 140/85 mm Hg. Physical examination shows nontender, erythematous macules on the palms and soles. A photograph of one of his fingernails is shown. Microscopic examination of the nail lesion is most likely to show which of the following?
A 73-year-old man presents to your clinic for a routine checkup. His medical history is notable for a previous myocardial infarction. He states that he has not seen a doctor in "many years". He has no complaints. When you auscultate over the cardiac apex with the bell of your stethoscope, you notice an additional sound immediately preceding S1. This extra heart sound is most likely indicative of which of the following processes?
A 32-year-old woman comes to the physician because of a 3-month history of recurrent headaches and nausea. The headaches occur a few times a month and alternately affect the right or left side. The headaches are exacerbated by loud sounds or bright light. She is in graduate school and has been under a lot of stress recently. She does not smoke or drink alcohol but does drink 2–3 cups of coffee daily. Her only medication is an oral contraceptive. Physical examination shows no abnormalities; visual acuity is 20/20. Which of the following is the most likely diagnosis?
A 35-year-old man presents to his primary care provider complaining of dull pain in his scrotum and lower back pain over the last 3 months. He is a computer engineer working in a private IT company. He had an uncomplicated appendectomy at the age of 22 years, but is otherwise without a significant past medical history. He smokes 2–3 cigarettes on weekends and drinks alcohol occasionally. He is sexually active with his wife. Today his heart rate is 90/min and blood pressure is 132/76 mm Hg. Scrotal examination reveals a firm, small and painless nodule on the left testicle. Scrotal ultrasound reveals a 0.9 x 0.5 cm irregular, non-cystic mass. He undergoes a left radical orchiectomy and histopathological examination reveals uniform tumor cells with abundant clear cytoplasm and distinct cell borders, consistent with a seminoma. Subsequent PET/CT scans show supraclavicular and para-aortic lymph node involvement. Which is the next and most appropriate step in the management of this patient?
A 72-year-old woman comes to the physician because of a 1-month history of progressive fatigue and shortness of breath. Physical examination shows generalized pallor. Laboratory studies show: Hemoglobin 5.8 g/dL Hematocrit 17% Mean corpuscular volume 86 μm3 Leukocyte count 6,200/mm3 with a normal differential Platelet count 240,000/mm3 A bone marrow aspirate shows an absence of erythroid precursor cells. This patient’s condition is most likely associated with which of the following?
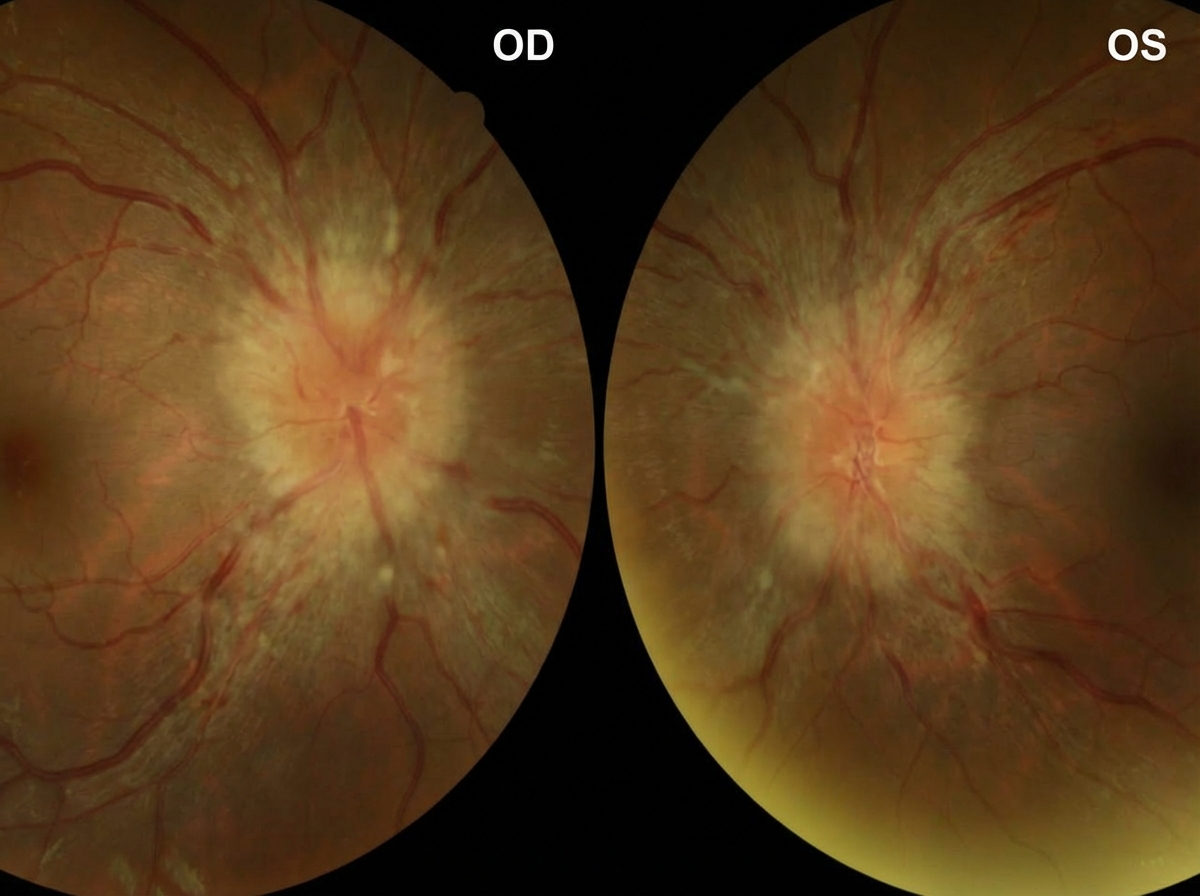
A 22-year-old woman comes to the emergency department because of frontal throbbing headaches for 3 weeks. Yesterday, the patient had blurry vision in both eyes and a brief episode of double vision. She has been taking ibuprofen with only mild improvement of her symptoms. She has polycystic ovarian syndrome, type 2 diabetes mellitus, and facial acne. She has not had any trauma, weakness, or changes in sensation. Her current medications include metformin and vitamin A. She is 158 cm (5 ft 2 in) tall and weighs 89 kg (196 lbs); BMI is 36 kg/m2. Vital signs are within normal limits. Examination shows decreased peripheral vision. Fundoscopic examination of both eyes is shown. MRI of the brain shows an empty sella. Which of the following is the most appropriate next step in management?
A 51-year-old woman comes to the physician because of fatigue and progressive pain and stiffness in her hands for 3 months. She used to play tennis but stopped 1 month ago because of difficulties holding the racket and her skin becoming “very sensitive to sunlight.” Her last menstrual period was 1 year ago. She has diabetes mellitus controlled with insulin. She does not smoke or drink alcohol. Vital signs are within normal limits. The patient appears tanned. The second and third metacarpophalangeal joints of both hands are tender to palpation and range of motion is limited. Which of the following is the most appropriate next step in diagnosis?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app