
Cardiology — MCQs

On this page
A 70-year-old man with hypertension and type 2 diabetes mellitus is admitted to the hospital 8 hours after the onset of impaired speech and right-sided weakness. Two days after admission, he becomes confused and is difficult to arouse. His pulse is 64/min and blood pressure is 166/96 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 95%. Fundoscopic examination shows bilateral optic disc swelling. He is intubated and mechanically ventilated. A CT scan of the brain shows hypoattenuation in the territory of the left middle cerebral artery with surrounding edema and a 1-cm midline shift to the right. Which of the following interventions is most likely to result in a decrease in this patient's intracranial pressure?
A 39-year-old woman with a history of migraine headaches is brought to the emergency room because of a severe, sudden-onset, throbbing headache and double vision for 1 hour. She says that she has been having frequent headaches and has not had her period in several months. Her blood pressure is 93/61 mm Hg. Visual field testing shows decreased visual acuity and bilateral temporal visual field defects. Which of the following is the most likely diagnosis?
A 67-year-old male presents to his primary care physician complaining of increased fatigue over the last year. He also says that his friends say he appears to be more pale. His past medical history is significant for 10 years of arthritis. Physical exam reveals conjunctival pallor. Based on clinical suspicion RBC tests are ordered showing a mean corpuscular volume (MCV) of 75 fl (normal 80-100 fl) and a peripheral blood smear is obtained and found to be normal. Iron studies show a serum iron of 30 micromolar (normal range 50-170) and a serum ferritin of 300 micrograms/liter (normal range 15-200). What is the most likely diagnosis in this patient?
A 55-year-old patient is brought to the emergency department because he has had sharp chest pain for the past 3 hours. He reports that he can only take shallow breaths because deep inspiration worsens the pain. He also reports that the pain increases with coughing. Two weeks ago, he underwent cardiac catheterization for an acute myocardial infarction. Current medications include aspirin, ticagrelor, atorvastatin, metoprolol, and lisinopril. His temperature is 38.54°C (101.1°F), pulse is 55/min, respirations are 23/min, and blood pressure is 125/75 mm Hg. Cardiac examination shows a high-pitched scratching sound best heard when the patient is sitting upright and during expiration. An ECG shows diffuse ST elevations and ST depression in aVR and V1. An echocardiography shows no abnormalities. Which of the following is the most appropriate treatment in this patient?
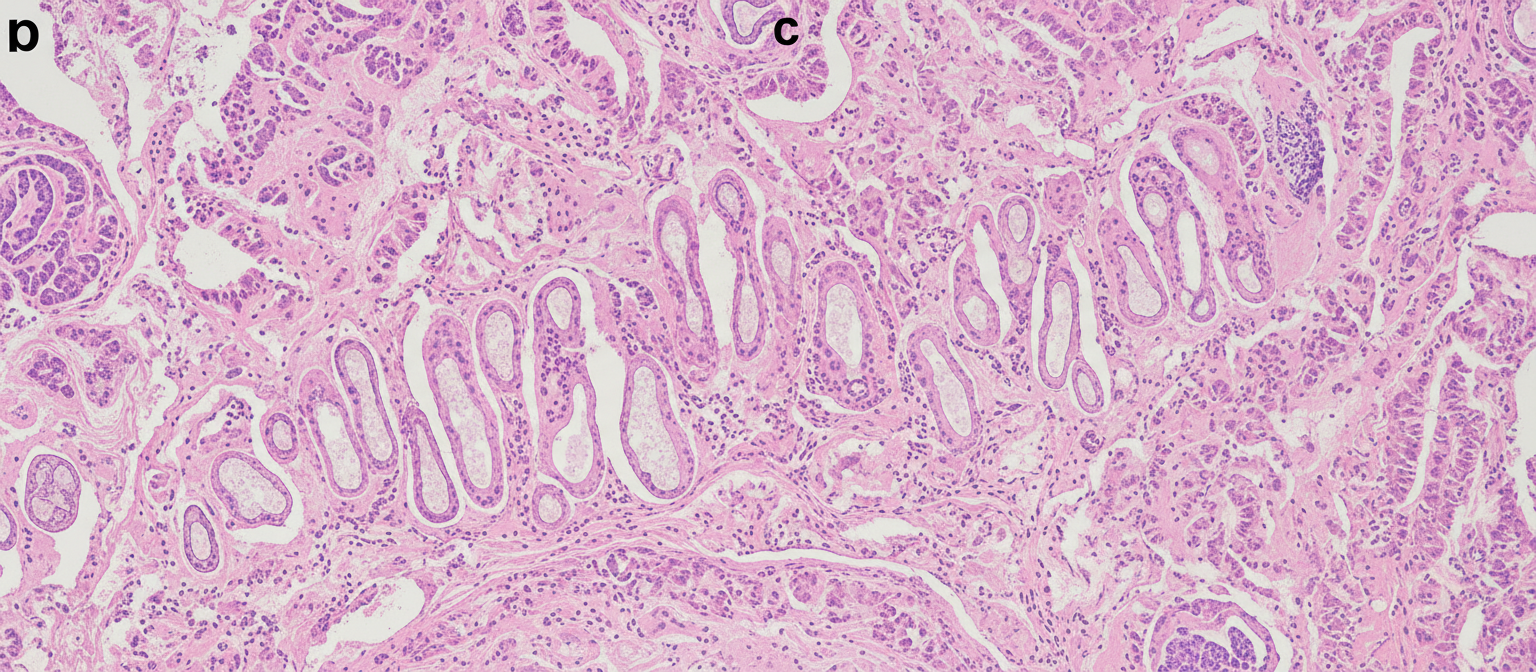
A 69-year-old woman presents to her physician’s office with cough, increasing fatigue, and reports an alarming loss of 15 kg (33 lb) weight over the last 4 months. She says that she has observed this fatigue and cough to be present over the past year, but pushed it aside citing her age as a reason. The cough has been progressing and the weight loss is really worrying her. She also observed blood-tinged sputum twice over the last week. Past medical history is noncontributory. She does not smoke and does not use recreational drugs. She is relatively active and follows a healthy diet. Today, her vitals are normal. On examination, she appears frail and pale. At auscultation, her lung has a slight expiratory wheeze. A chest X-ray shows a coin-shaped lesion in the periphery of the middle lobe of the right lung. The nodule is biopsied by interventional radiology (see image). Which of the following types of cancer is most likely associated with this patient’s symptoms?
A 30-year-old man with Down syndrome is brought to the physician by his mother for the evaluation of fatigue. Physical examination shows bluish-colored lips and digital clubbing that were not present at his most recent examination. Right heart catheterization shows a right atrial pressure of 32 mmHg. Which of the following is most likely involved in the pathogenesis of this patient's current condition?
A 35-year-old woman presents to the ER with shortness of breath, cough, and severe lower limb enlargement. The dyspnea was of sudden onset, started a week ago, and increased with exercise but did not disappear with rest. Her cough was dry, persistent, and non-productive. She has a family history of maternal hypertension. Her vital signs include heart rate 106/min, respiratory rate 28/min, and blood pressure 140/90 mm Hg. On physical examination, thoracic expansion was diminished on the right side with rhonchi and crackles on the lower two-thirds of both sides, with left predominance. A systolic murmur was heard on the tricuspid foci, which increased in intensity with inspiration. There was jugular engorgement when the bed was placed at 50°. Palpation of the abdomen was painful on the right hypochondrium, with hepatomegaly 4 cm below the lower costal edge. Hepatojugular reflux was present. Soft, painless, pitting edema was present in both lower limbs up until the middle third of both legs. Lung computed tomography (CT) and transthoracic echocardiogram were performed and detected right heart failure and severe pulmonary fibrosis. What is the most likely diagnosis?
A 33-year-old man presents to the emergency department with dizziness. He states he has experienced a sustained sense of disequilibrium for the past 2 days. He feels that the floor is unstable/moving. The patient is otherwise healthy and does not have any other medical diagnoses. The patient is currently taking vitamin C as multiple family members are currently ill and he does not want to get sick. His temperature is 98.1°F (36.7°C), blood pressure is 120/83 mmHg, pulse is 73/min, respirations are 16/min, and oxygen saturation is 98% on room air. Physical exam is notable for a horizontal nystagmus. The Dix-Hallpike maneuver does not provoke symptoms and examination of the patient’s cranial nerves is unremarkable. Which of the following is the most likely diagnosis?
A 35-year-old woman comes to the physician because of fatigue and a 9-kg (20-lb) weight gain over the past 12 months. She also has irregular menstrual cycles and difficulty sleeping. Menses occur at irregular 35- to 50-day intervals and last 3–7 days. Menarche was at age of 13 years and her last menstrual period was 4 weeks ago. She has 1-year history of hypertension treated with hydrochlorothiazide. She drinks a glass of wine daily. She is 163 cm (5 ft 4 in) tall and weighs 85 kg (187 lb); BMI is 32 kg/m2. Her temperature is 37°C (98.6°F), pulse is 82/min, respirations are 16/min, and blood pressure is 125/86 mm Hg. Examination shows acne on the face and hair on the chin and around the umbilicus. The face has a rounded shape and is reddened. There are several smaller bruises on both forearms. This patient is most likely to have which of the following findings?
A 25-year-old woman comes to the physician because of a 4-month history of anxiety and weight loss. She also reports an inability to tolerate heat and intermittent heart racing for 2 months. She appears anxious. Her pulse is 108/min and blood pressure is 145/87 mm Hg. Examination shows a fine tremor of her outstretched hands. After confirmation of the diagnosis, the patient is scheduled for radioactive iodine ablation. At a follow-up visit 2 months after the procedure, she reports improved symptoms but new-onset double vision. Examination shows conjunctival injections, proptosis, and a lid lag. Slit-lamp examination shows mild corneal ulcerations. The patient is given an additional medication that improves her diplopia and proptosis. Which of the following mechanisms is most likely responsible for the improvement in this patient's ocular symptoms?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app