
Cardiology — MCQs

On this page
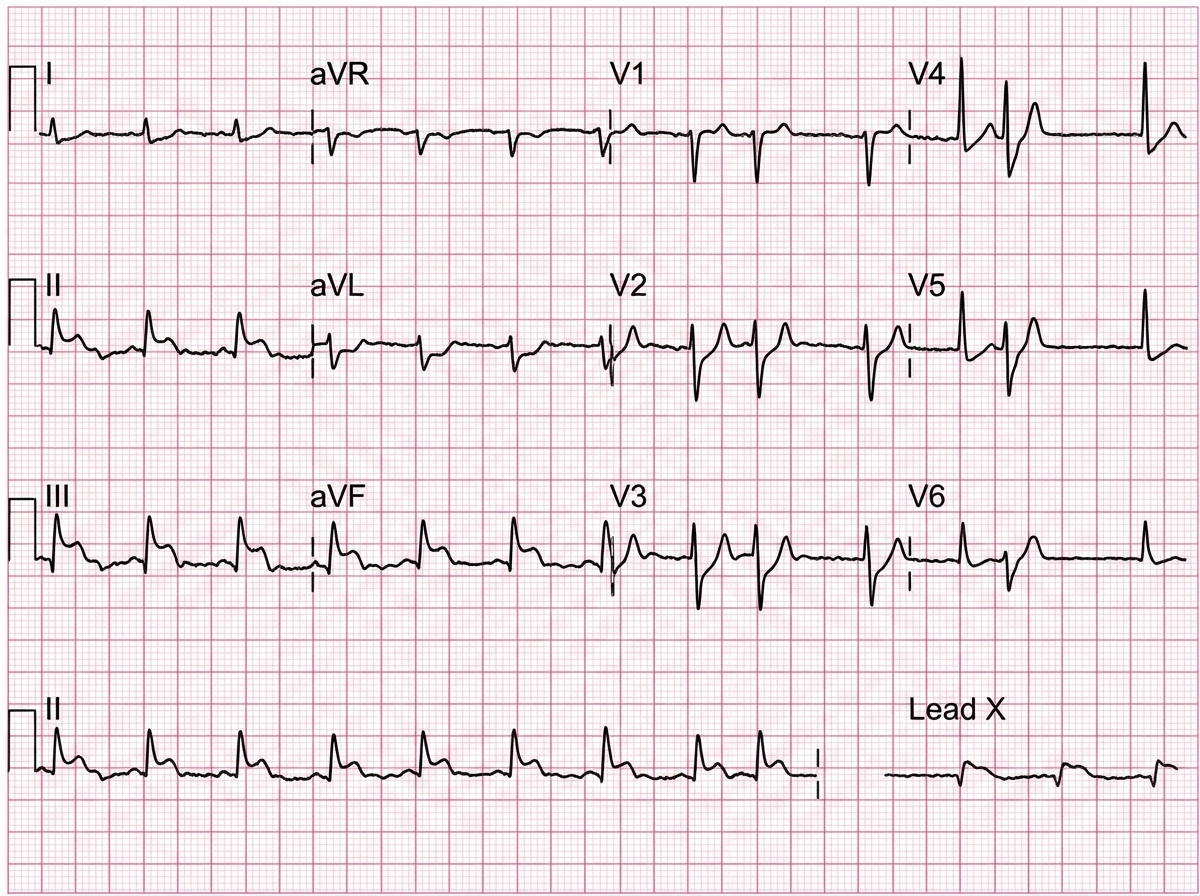
A 16-year-old boy has a history of recurrent episodes of fainting in school assembly. ECG was done. Which is incorrect about the condition?
A 65-year-old man presents with crushing chest pain for 2 hours. On examination, BP = 80/60 mm Hg and JVP is elevated 4 cm above the sternal angle. All are true about the condition shown except:
A 40-year-old man who had recently joined a gym collapsed on the treadmill. His resting ECG shows a normal QTc and cardiac imaging shows no structural heart disease. He was rushed to the hospital where an ECG shows presence of:

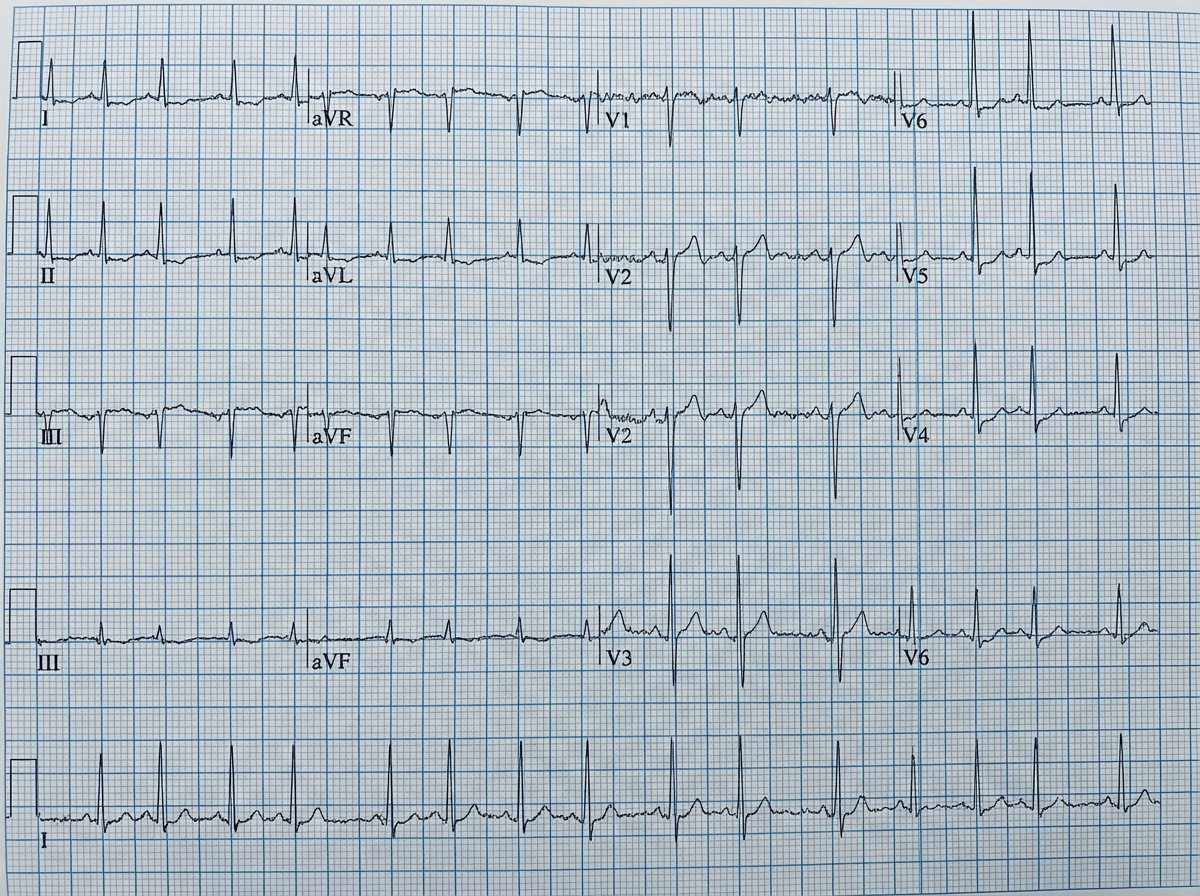
A 70-year-old hypertension patient presents with complaints of palpitations and presyncope. On examination, his heart rate is 72 bpm and BP is 150/100, ECG done shows:
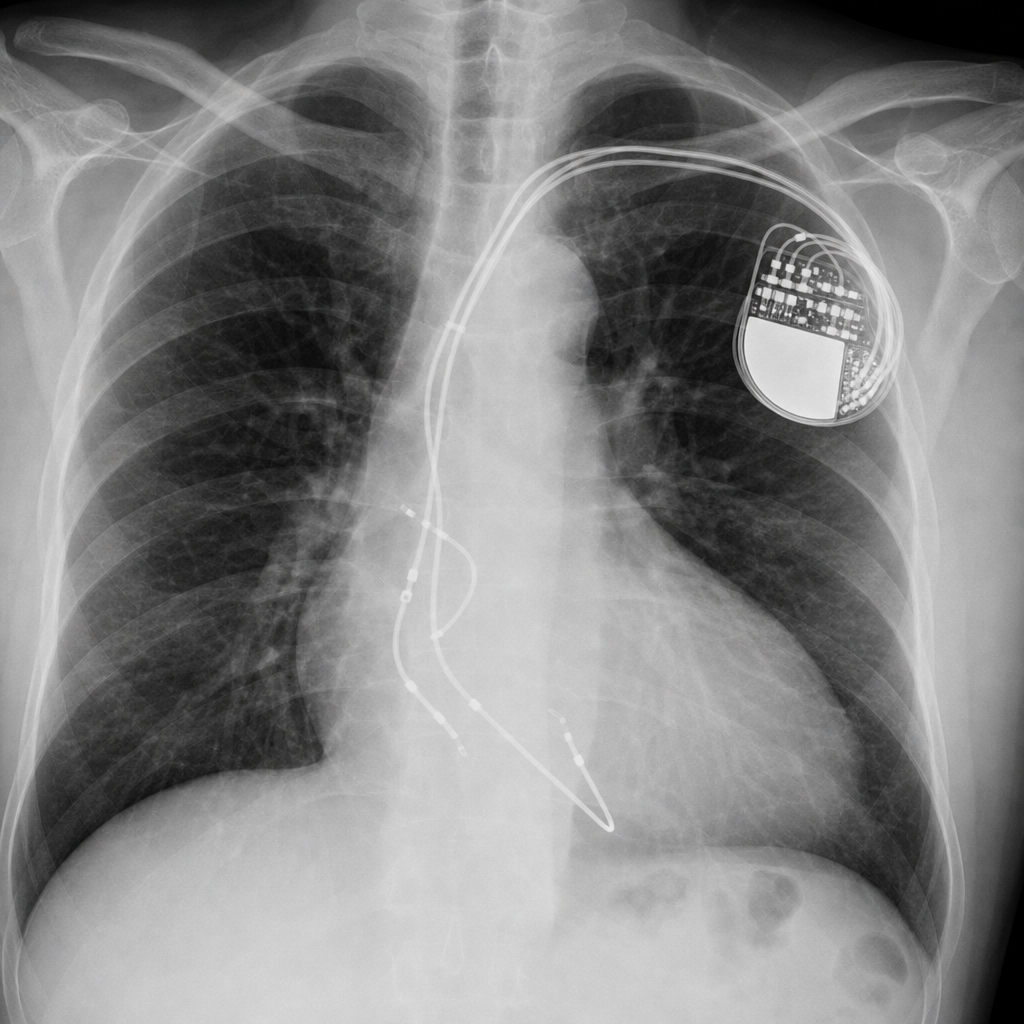
A 50-year-old dilated cardiomyopathy patient underwent a procedure shown below. What is it known as?
This 50-year-old patient developed syncope after having a coffee and is currently unresponsive and hypotensive with sustained polymorphic ventricular tachycardia. ECG was done .Which is the most appropriate therapy for a patient suffering from the condition shown below?

A patient suffers from STEMI. He was taken to cath lab. What is the name of the Catheter shown below?

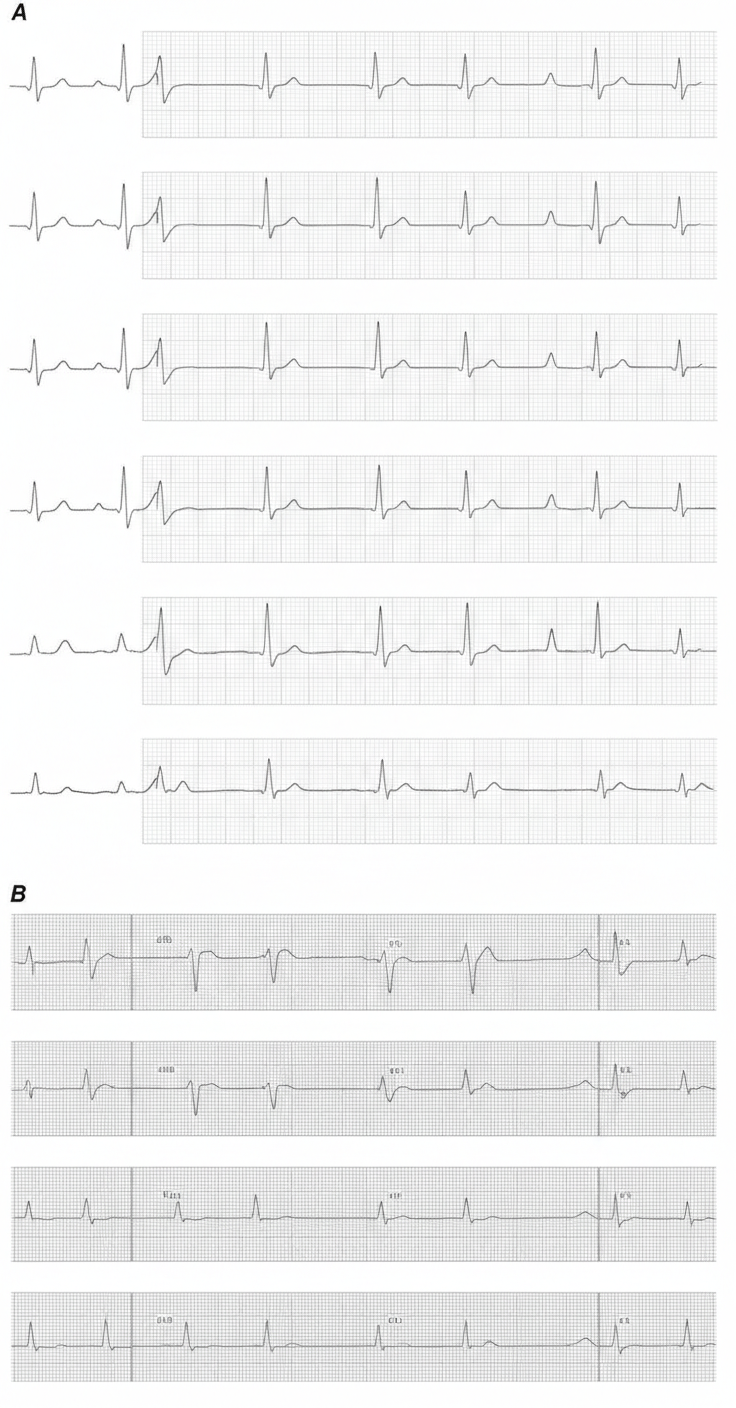
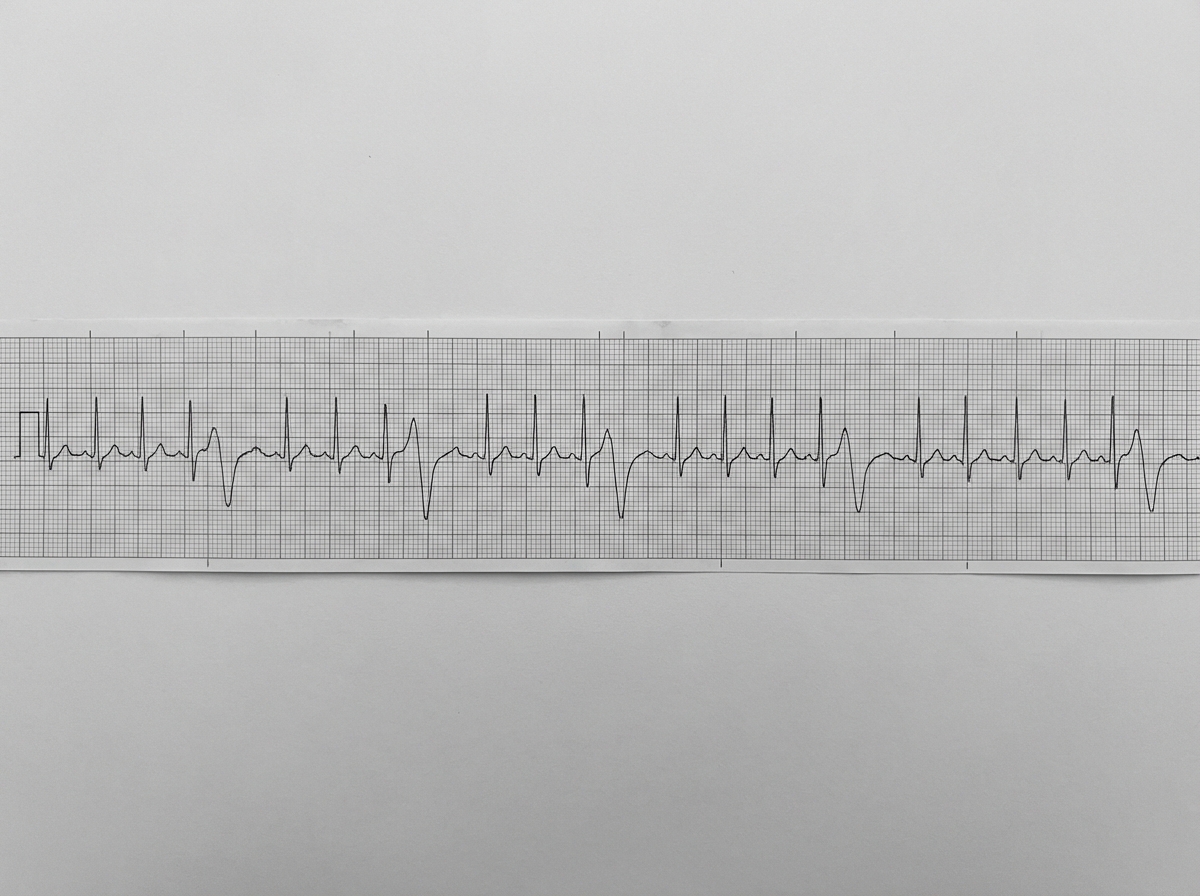
The tracing shows a repeating pattern of three normal sinus beats followed by a premature ventricular contraction. This is diagnostic of:
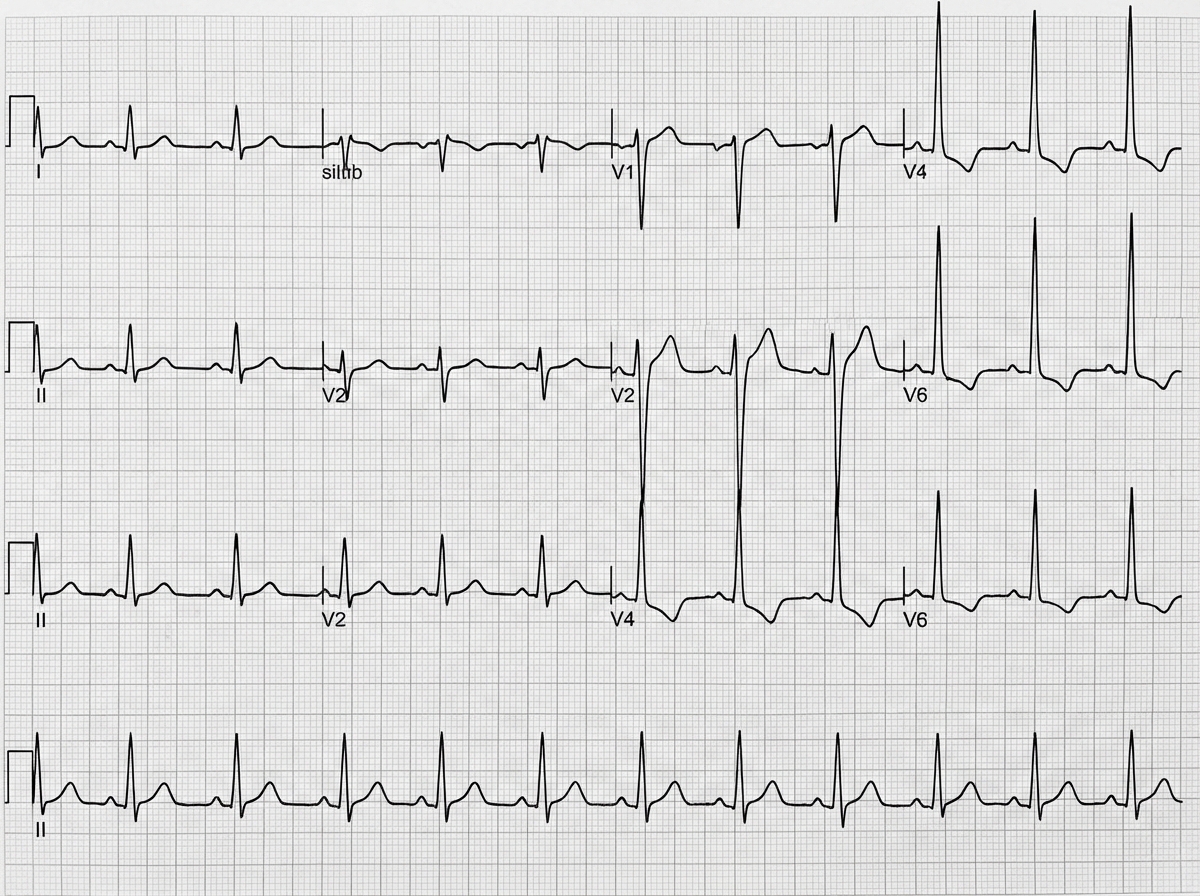
A 65-year-old pensioner in ESI dispensary complains of exercise intolerance. On auscultation a systolic murmur grade 3 is heard. What does the ECG show?
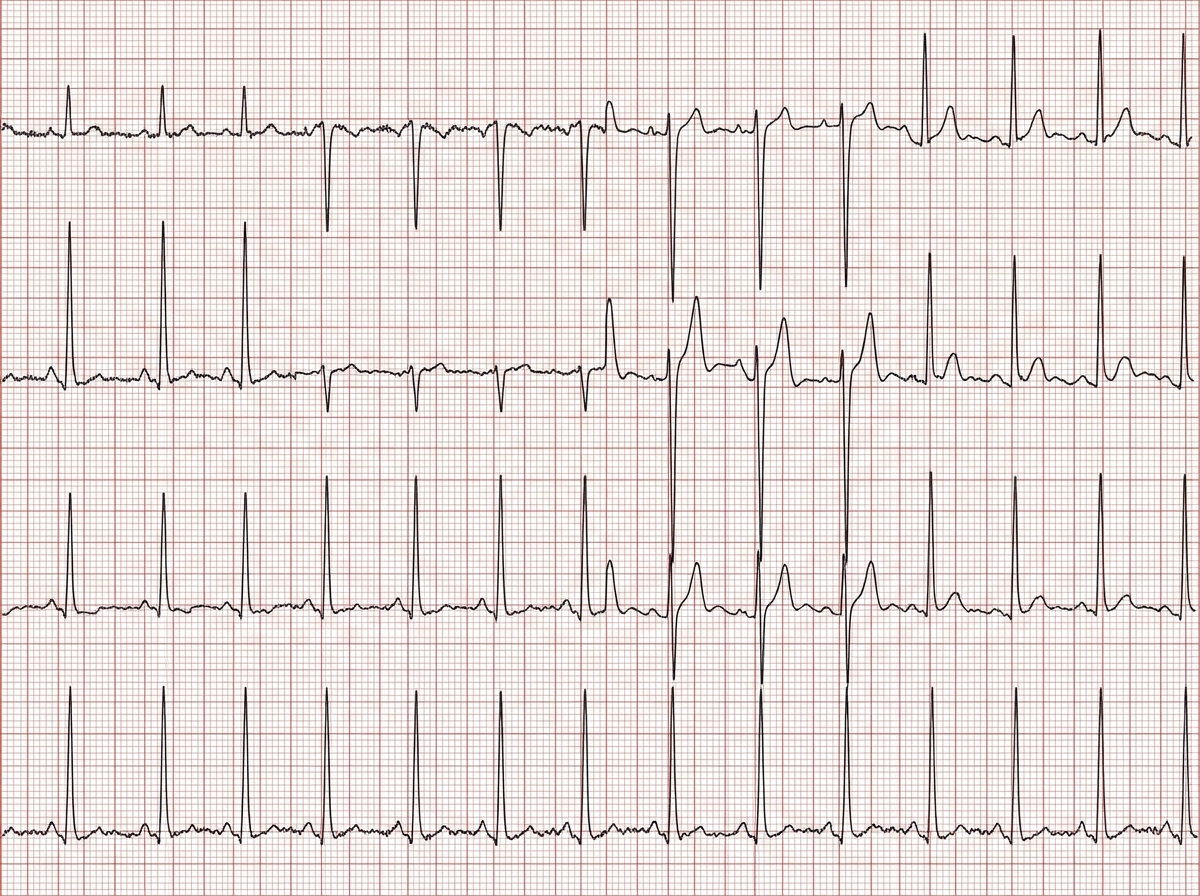
An 89-year-old man with hypertension presents for routine follow-up. ECG shows:
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app