
Cardiology — MCQs

On this page
A 64-year-old man presents to his primary care physician for 4 weeks of recurrent fever, night sweats, malaise, and fatigue. Associated with shortness of breath and orthopnea. Family and personal history are unremarkable, though an echocardiogram performed 2 years ago demonstrated billowing of a mitral leaflet beyond the mitral annular plane with mild valvular incompetence. Upon physical examination, he is found with a blood pressure of 100/68 mm Hg, a heart rate of 98/min, a respiratory rate of 20/min, and a body temperature of 38.5°C (101.3°F). Cardiopulmonary auscultation reveals a high-pitched holosystolic murmur over the cardiac apex that radiates to the left axilla. Skin lesions are found on the patient's palms: multiple painless, nonblanching erythematous macules scattered over the thenar eminence and central palm. Which of the following entities predisposed this patient's condition?

A 44-year-old woman is brought to the emergency department for confusion and lethargy for the past 2 hours. Per the husband, the patient was behaving weirdly and forgot how to get to the bathroom at her house. She was also difficult to wake up from her nap. The husband denies any fever, weight loss, headaches, dizziness, chest pain, or gastrointestinal changes. He reports that she had frequent diarrhea over the past 3 days but attributed it to food poisoning. In the emergency room, the patient had a 1-minute episode of seizure activity. Following initial resuscitation and stabilization, laboratory studies were performed and the results are shown below. Hemoglobin: 13 g/dL Hematocrit: 38% Leukocyte count: 7,600/mm^3 with normal differential Platelet count: 170,000/mm^3 Serum: Na+: 125 mEq/L Cl-: 90 mEq/L K+: 3.2 mEq/L HCO3-: 20 mEq/L BUN: 22 mg/dL Glucose: 101 mg/dL Creatinine: 1.0 mg/dL Thyroid-stimulating hormone: 3.2 µU/mL Ca2+: 9.3 mg/dL AST: 19 U/L ALT: 22 U/L What is the most appropriate treatment for this patient?
A 61-year-old man with a past medical history significant for asthma and psoriasis presents to the clinic for a wellness visit. He has no specific complaints. The patient’s blood pressure is 121/73 mm Hg, the pulse is 81/min, the respiratory rate is 16/min, and the temperature is 37.2°C (99.1°F). Physical examination reveals a 3.3 cm (1.2 in) lesion overlying his left elbow with an erythematous border, covered with a silver scale. What type of lesion is on the patient’s elbow?
A 74-year-old man comes to the attention of the inpatient hospital team because he started experiencing shortness of breath and left-sided back pain 3 days after suffering a right hip fracture that was treated with hip arthroplasty. He says that the pain is sharp and occurs with deep breathing. His past medical history is significant for diabetes and hypertension for which he takes metformin and lisinopril. On physical exam, he is found to have a friction rub best heard in the left lung base. His right calf is also swollen with erythema and induration. Given this presentation, which of the following most likely describes the status of the patient's lungs?
A 35-year-old woman comes to the clinic with complaints of joint pain and stiffness for the past few months. Her hands, lower back, and left knee are involved and associated with morning stiffness that improves throughout the day with activities. She also complains that her fingers change color upon exposure to cold. She has also noticed a tightening of the skin on her face and thinning of her lips. She feels tired throughout the day and has taken over-the-counter multivitamins that do not seem to help her much. The patient does not smoke cigarettes and drinks alcohol socially. She was diagnosed with hypertension 1 year ago and has been taking hydralazine for the past year. She lost her parents in a road traffic accident 3 years ago. Temperature is 36.7°C (98°F), blood pressure is 140/85 mm Hg, pulse is 72/min, respirations are 12/min, and BMI is 25 kg/m2. Her skin appears shiny and slightly thickened, especially her face and hands. Laboratory investigation: Complete blood count Hemoglobin 9.5 g/dl Leucocytes 5,500/mm3 Platelets 150,000/mm3 ANA positive Anti-centromere Antibody negative Anti Scl-70 positive Anti Jo-1 negative Anti-histone negative Anti DsDNA negative What is the most likely diagnosis in this patient?
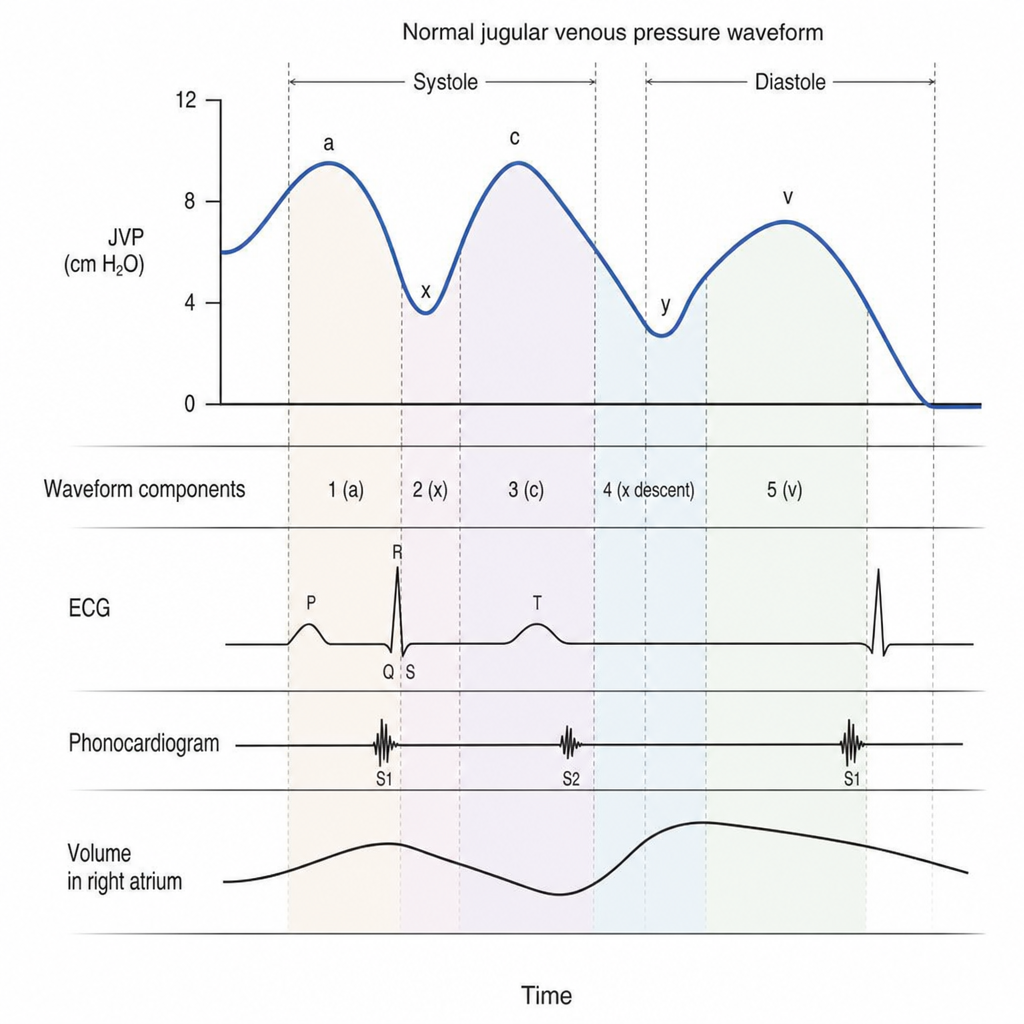
A 57-year-old woman comes to the physician because of a 2-month history of intermittent dyspnea and dizziness. She has a history of mitral valve stenosis. Her pulse is 125/min and irregularly irregular, and blood pressure is 102/66 mm Hg. A transthoracic echocardiogram shows doming of the anterior mitral valve leaflet during diastole. Which of the following elements is most likely to be absent from this patient's jugular venous pressure waveform?
A 73-year-old female is hospitalized following a pelvic fracture. She undergoes surgical repair without complication. Four days into her hospital stay, she develops acute dyspnea and chest pain accompanied by oxyhemoglobin desaturation. Which of the following arterial blood gas values is the patient most likely to have? (normal values: pH 7.35 - 7.45, PaO2 80 - 100 mm Hg, PaCO2 35-45 mm Hg, HCO3 22-26)
A 39-year-old female with a long history of major depressive disorder presents to the emergency room with altered mental status. Her husband found her on the floor unconscious and rushed her to the emergency room. He reports that she has been in a severe depressive episode over the past several weeks. Vital signs are temperature 38.1 degrees Celsius, heart rate 105 beats per minute, blood pressure 110/70, respiratory rate 28, and oxygen saturation 99% on room air. Serum sodium is 139, chloride is 100, and bicarbonate is 13. Arterial blood gas reveals a pH of 7.44 with a pO2 of 100 mmHg and a pCO2 of 23 mmHg. Which of the following correctly identifies the acid base disorder in this patient?
A 32-year-old woman presents to the emergency department due to severe, intractable headaches, and bilateral ocular pain. Her symptoms began approximately 2 weeks prior to presentation and have progressively worsened. She initially had right-sided headaches that were sharp, interfered with sleep, and were unresponsive to pain medications. The headache was around her right eye and cheek, and she noticed diplopia with right lateral gaze. Her symptoms were accompanied by fatigue, fever, and edema around the right eye. Approximately 2 days after these symptoms, she developed swelling around the left eye. Medical history is significant for a recent rhinosinusitis infection. Her temperature is 101°F (38.3°C), blood pressure is 133/72 mmHg, pulse is 90/min, and respirations are 18/min. On physical exam, there is ptosis, proptosis, chemosis, and periorbital swelling of both eyes. There is hyperesthesia in the bilateral ophthalmic and maxillary divisions of the trigeminal nerve. Fundoscopic exam demonstrates bilateral papilledema. There is mydriasis and eye muscle weakness in all directions. Which of the following is the most likely diagnosis?
A 68-year-old man is referred to the cardiology department with complaints of shortness of breath on exertion that has been progressive for the last 6 months. He has a history of diabetes mellitus type II which is controlled with diet alone. He has a temperature of 37.1℃ (98.8℉), the pulse is 76/min, and the blood pressure is 132/86 mm Hg. Physical examination is notable for a systolic murmur heard best at the right upper sternal border with radiation to the carotid arteries. ECG shows left ventricular hypertrophy and absent Q waves. Transthoracic echocardiogram shows an elevated aortic pressure gradient with severe leaflet calcification and left ventricular diastolic dysfunction. Which of the following has a survival benefit for this patient’s cardiac problem?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app