
Cardiology — MCQs

On this page
A 27-year-old male with a history of injection drug use has been feeling short of breath and fatigued for the past several weeks. He is having trouble climbing the stairs to his apartment and occasionally feels like his heart is racing out of control. His past medical history is most notable for a previous bout of infective endocarditis after which he was lost to follow-up. On exam, you note that his carotid pulse has rapid rise and fall. Which of the following would you also expect to find?
A 72-year-old man presents to the emergency department for a change in his behavior. The patient's wife called 911 and he was brought in by emergency medical services. She noticed that he seemed somnolent and not very responsive. The patient has a past medical history of type II diabetes, obesity, osteoarthritis, and migraine headaches. His current medications include naproxen, insulin, atorvastatin, metformin, ibuprofen, omeprazole, and fish oil. His temperature is 99.5°F (37.5°C), blood pressure is 170/115 mmHg, pulse is 80/min, respirations are 19/min, and oxygen saturation is 98% on room air. On physical exam, the patient is somnolent and has a Glasgow Coma Scale of 11. Cardiac and pulmonary exams are notable for bibasilar crackles and a systolic murmur that radiates to the carotids. Neurological exam is deferred due to the patient's condition. Laboratory values are shown below. Hemoglobin: 12 g/dL Hematocrit: 36% Leukocyte count: 9,500 cells/mm^3 with normal differential Platelet count: 199,000/mm^3 Serum: Na+: 144 mEq/L Cl-: 98 mEq/L K+: 4.0 mEq/L HCO3-: 16 mEq/L BUN: 44 mg/dL Glucose: 202 mg/dL Creatinine: 2.7 mg/dL Ca2+: 9.2 mg/dL AST: 12 U/L ALT: 22 U/L The patient is started on IV fluids. Which of the following represents the best next step in management?
A 49-year-old woman comes to the physician because of a 4-month history of a dry cough and shortness of breath on exertion. She also reports recurrent episodes of pain, stiffness, and swelling in her wrist and her left knee over the past 6 months. She had two miscarriages at age 24 and 28. Physical examination shows pallor, ulcerations on the palate, and annular hyperpigmented plaques on the arms and neck. Fine inspiratory crackles are heard over bilateral lower lung fields on auscultation. Which of the following additional findings is most likely in this patient?
A 29-year-old woman, gravida 1, para 0 at 11 weeks' gestation comes to the physician because of a 2-day history of left lower extremity pain and swelling. Her temperature is 37.9°C (100.2°F). Physical examination shows a tender, palpable cord on the lateral aspect of the left lower leg. The overlying skin is erythematous and indurated. Duplex ultrasound shows vascular wall thickening and subcutaneous edema. Which of the following is the most likely diagnosis?
A 34-year-old woman comes to the emergency department with midsternal chest pain, shortness of breath, and cough with bloody sputum for the past 3 hours. The pain started after moving furniture at home and worsens when taking deep breaths. The patient has a history of hypertension. She has smoked one pack of cigarettes daily for the past 20 years. She drinks 1–2 glasses of wine per day. Current medications include enalapril and an oral contraceptive. Her temperature is 38.2°C (100.8°F), pulse is 110/min, respirations are 20/min, and blood pressure is 110/70 mm Hg. Oxygen saturation is 92% on room air. Physical examination shows decreased breath sounds over the left lung base. There is calf pain on dorsal flexion of the right foot. Examination of the extremities shows warm skin and normal pulses. Further evaluation of this patient is most likely to show which of the following findings?
A 38-year-old man comes to the physician because of fever, malaise, productive cough, and left-sided chest pain for 2 weeks. During this time, he has woken up to a wet pillow in the morning on multiple occasions and has not been as hungry as usual. He was diagnosed with HIV infection 1 year ago. He currently stays at a homeless shelter. He has smoked one pack of cigarettes daily for 22 years. He has a history of intravenous illicit drug use. He drinks 5–6 beers daily. He is receiving combined antiretroviral therapy but sometimes misses doses. His temperature is 38.6°C (101.5°F), pulse is 106/min, and blood pressure is 125/85 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 94%. Auscultation shows decreased breath sounds over the left base of the lung. There is dullness to percussion on the left lower part of the chest. Laboratory studies show: Hemoglobin 14 g/dL Leukocyte count 5,000/mm3 CD4+ T lymphocytes 240/mm3 (N > 500) Serum Creatinine 0.9 mg/dL γ-Glutamyltransferase (GGT) 65 U/L (N = 5–50) Aspartate aminotransferase (AST) 15 U/L Alanine aminotransferase (ALT) 19 U/L Alkaline phosphatase 40 U/L Lactate dehydrogenase (LDH) 50 U/L An x-ray of the chest shows a left-sided pleural effusion and hilar lymphadenopathy. Analysis of the pleural fluid shows an effusion with lymphocyte-predominant leukocytosis, high protein, an LDH of 500 U/L, and high adenosine deaminase. Which of the following is the most likely cause of this patient's condition?
A 44-year-old female is brought to the emergency room after losing consciousness at a shopping mall. Her husband states that they were shopping when the patient appeared sweaty and tremulous, became confused, then collapsed. She was unconscious for 5 minutes until a paramedic arrived. Fingerstick glucose at that time was 31 mg/dL and intramuscular glucagon was administered. The patient regained consciousness as she was being transported to the ambulance. On arrival in the emergency room, she is conscious but sleepy. She is able to report that her last meal prior to the mall was 5 hours ago. Her husband notes that over the last 3 months, she has complained of headaches and a milky discharge from both breasts, as well as nausea if she goes too long without eating. She works as an inpatient nurse and was exposed to tuberculosis 10 years ago but adequately treated. Because she was adopted as an infant, family history is unknown. Temperature is 98.4 deg F (36.9 deg C), blood pressure is 101/59 mmHg, pulse is 88/min, and respiration is 14/min. Preliminary lab values are shown below: Plasma glucose: 54 mg/dL Plasma insulin: 29 pmol/L (normal < 19 pmol/L) Plasma C-peptide: 272 pmol/L (normal < 200 pmol/L) Plasma proinsulin: 8 pmol/L (normal < 5 pmol/L) Plasma ß-hydroxybutyrate: 1.2 mmol/L (normal > 2.7 mmol/L after fasting) Which of the following is the most likely cause of this patient’s hypoglycemic episode?
A 48-year-old man comes to the physician for the evaluation of dyspnea and cough. He was diagnosed with esophageal cancer 10 months ago, for which he received radiochemotherapy. He has a history of atopic dermatitis and has smoked one pack of cigarettes daily for 30 years. Auscultation of the lungs shows decreased breath sounds bilaterally. Spirometry shows an FVC of 78% and an FEV1/FVC ratio of 95%. Which of the following is the most likely underlying condition?
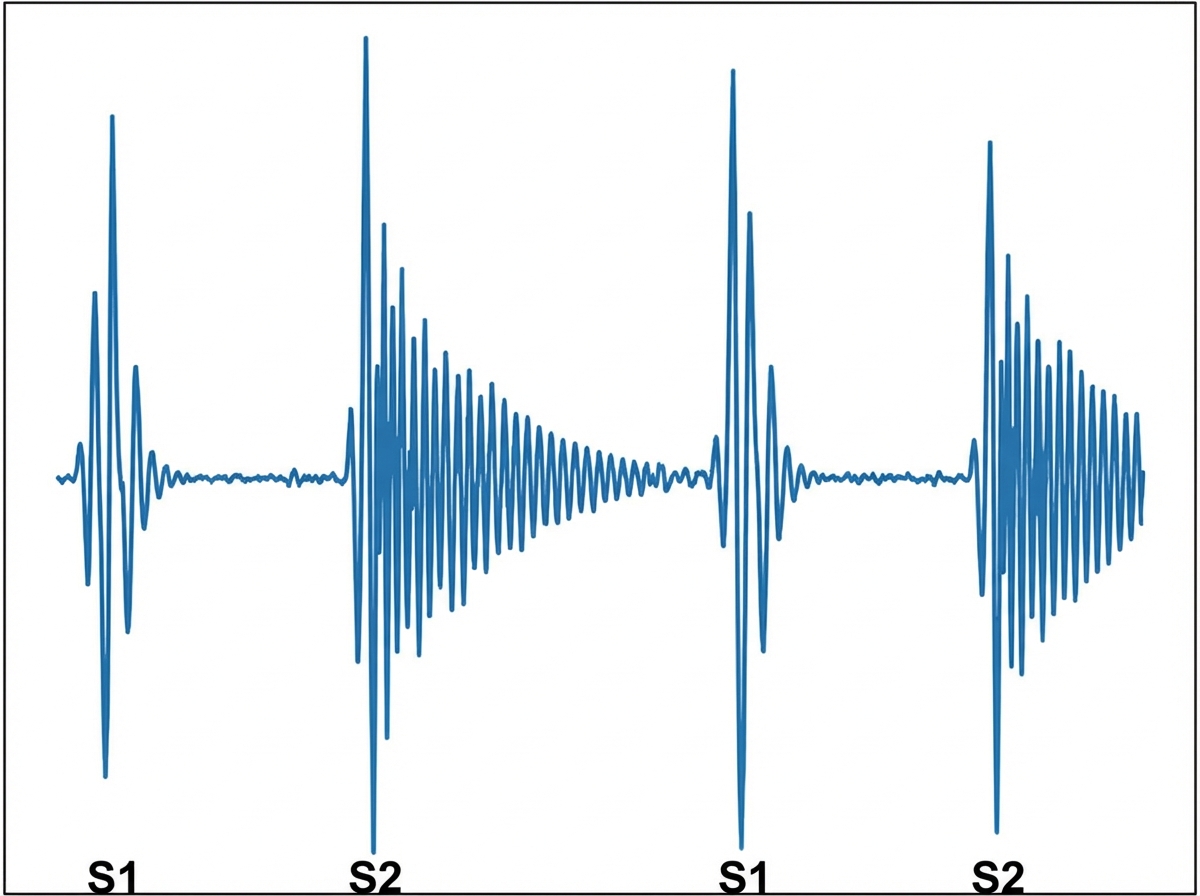
A 27-year-old man comes to the physician because of a 2-month history of palpitations and shortness of breath on exertion. He has no history of serious illness. He does not smoke or use illicit drugs. His pulse is 90/min, respirations are 18/min, and blood pressure is 140/40 mm Hg. Cardiac examination shows a murmur along the left sternal border. A phonocardiogram of the murmur is shown. Which of the following additional findings is most likely in this patient?
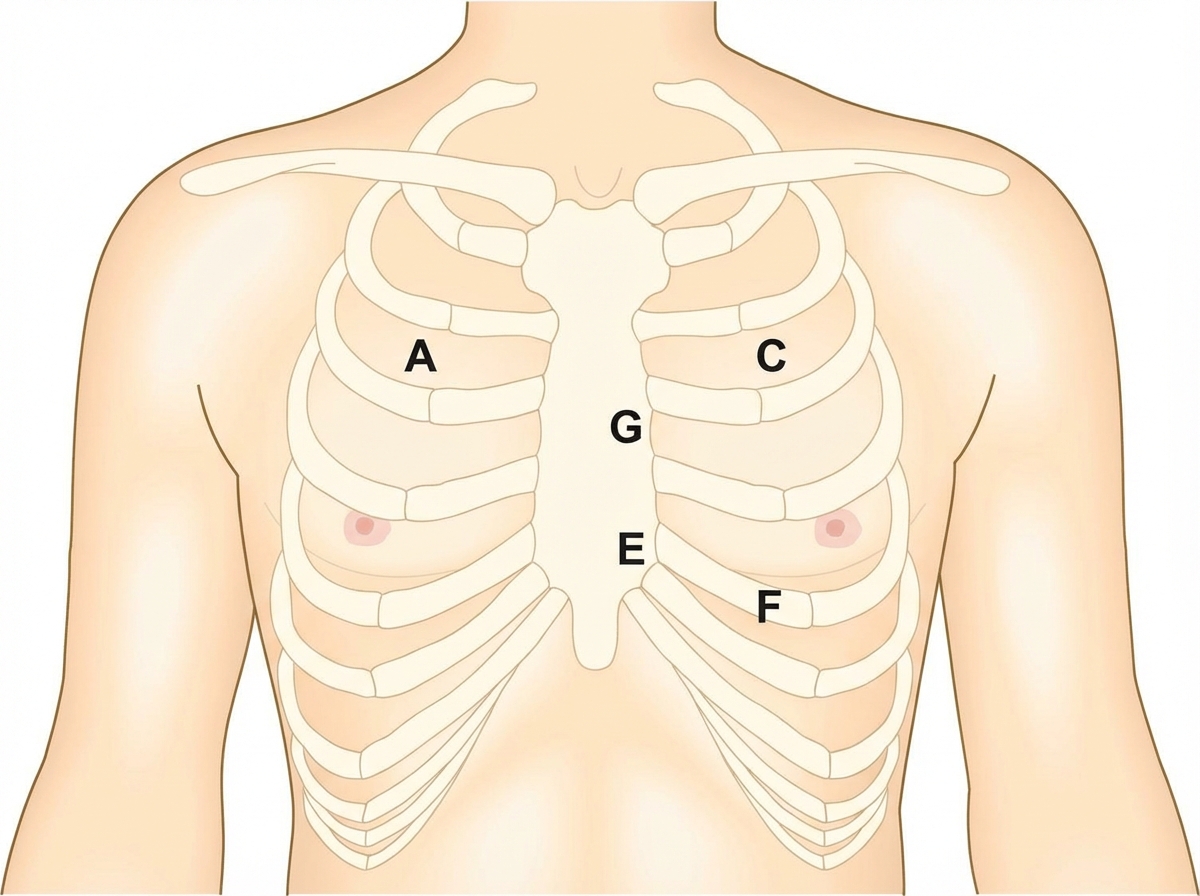
A 6-year-old boy is brought to the physician by his mother because of a 3-month history of episodic chest pain and shortness of breath on exertion. He is at the 99th percentile for height and 40th percentile for weight. Examination shows a high-arched palate, long and slender upper extremities, and elbows and knees that can be hyperextended. Cardiac examination shows a grade 2/6 late systolic, crescendo murmur with a midsystolic click. Over which of the following labeled areas is the murmur most likely to be heard best?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app