
Cardiology — MCQs

On this page
A 62-year-old woman comes to the physician in June for a routine check-up. She has chronic back pain and underwent an appendectomy at the age of 27. She is married and has two kids. The patient recently got back from a cruise to Mexico where she celebrated her 40th wedding anniversary. Her last mammogram was 6 months ago and showed no abnormalities. Her last Pap smear was 2 years ago and unremarkable. A colonoscopy 5 years ago was normal. Her mother died of breast cancer last year and her father has arterial hypertension. Her immunization records show that she has never received a pneumococcal or a shingles vaccine, her last tetanus booster was 6 years ago, and her last influenza vaccine was 2 years ago. She drinks 1– 2 alcoholic beverages every weekend. She takes a multivitamin daily and uses topical steroids. She regularly attends water aerobic classes and physical therapy for her back pain. She is 168 cm (5 ft 6 in) tall and weighs 72 kg (160 lb); BMI is 26 kg/m2. Her temperature is 36.7°C (98°F), pulse is 84/min, and blood pressure is 124/70 mm Hg. Which of the following is the most appropriate recommendation at this time?
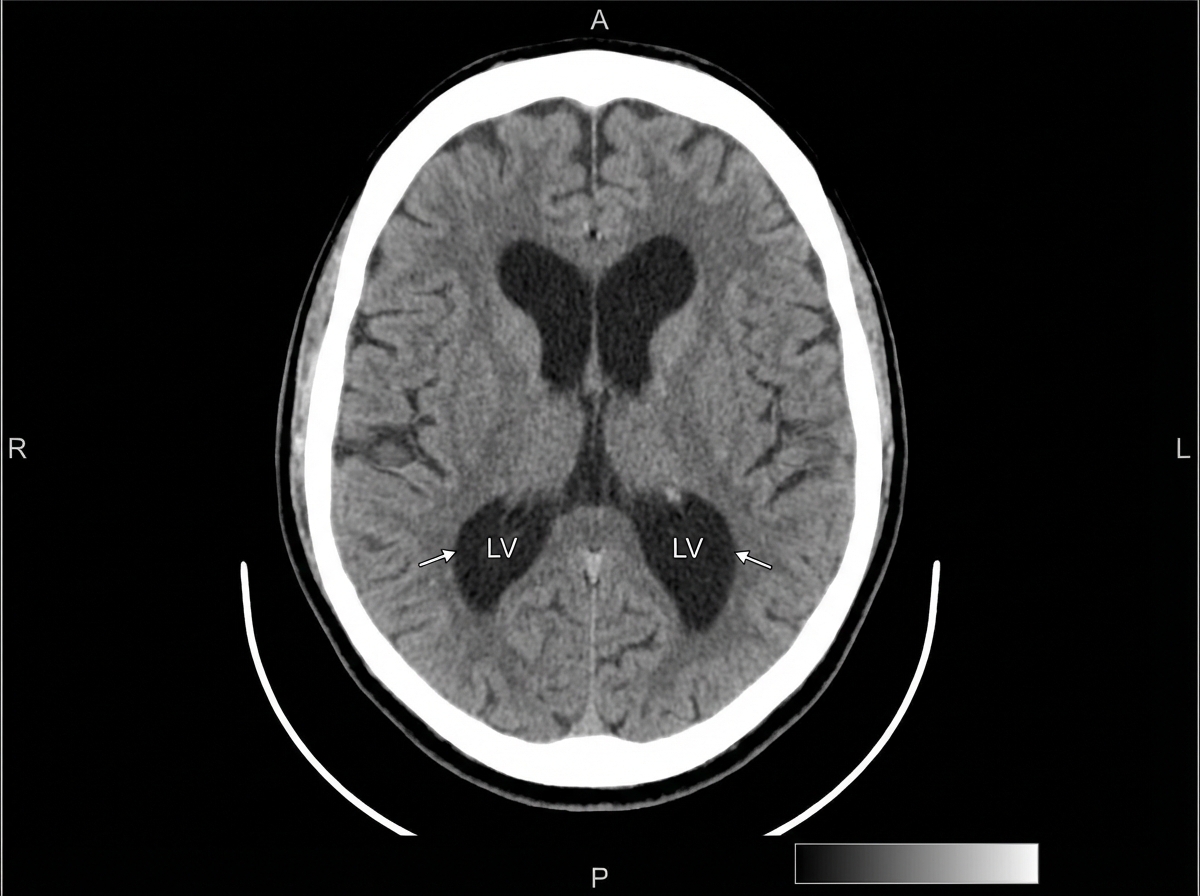
A 68-year-old woman in a wheelchair presents with her husband. She has a 12-month history of progressive difficulty in walking and maintaining balance. Her husband reports that she walks slowly, has difficulty turning, and her feet seem ‘glued to the ground’. She also has problems recalling names and details of recent events. She has no tremors, delusions, hallucinations, sleep disturbances, or head trauma. Past medical history is significant for essential hypertension treated with losartan and urinary incontinence, for which she takes oxybutynin. On physical examination, her vital signs include: temperature 37.0°C (98.6°F), blood pressure 130/70 mm Hg, and pulse 80/min. On neurologic examination, her gait is slow, with short steps and poor foot clearance. A head CT is shown. The patient undergoes a lumbar puncture to remove 50 ml of cerebrospinal fluid, which transiently improves her gait for the next 3 days. What is the next step in the management of this patient?
An 83-year-old woman with a past medical history of poorly controlled diabetes, hyperlipidemia, hypertension, obesity, and recurrent urinary tract infections is brought to the emergency room by her husband due to confusion, generalized malaise and weakness, nausea, and mild lower abdominal pain. Her medications include metformin and glyburide, atorvastatin, lisinopril, and hydrochlorothiazide. At presentation, her oral temperature is 38.9°C (102.2°F), the pulse is 122/min, blood pressure is 93/40 mm Hg, and oxygen saturation is 96% on room air. On physical examination, she is breathing rapid shallow breaths but does not have any rales or crackles on pulmonary auscultation. No murmurs are heard on cardiac auscultation and femoral pulses are bounding. Her skin is warm, flushed, and dry to touch. There is trace bilateral pedal edema present. Her abdomen is soft and non-distended, but she has some involuntary guarding on palpation of the suprapubic region. ECG shows normal amplitude sinus tachycardia without evidence of ST-segment changes or T-wave inversions. Which of the following would most likely be the relative pulmonary artery catheterization measurements of pulmonary capillary wedge pressure (PCWP), mixed venous oxygen saturation (SvO2), calculated cardiac output (CO), and systemic vascular resistance (SVR) in this patient?
A 59-year-old patient with COPD is admitted with difficulty breathing and increased sputum production. Approx. a week ago, he developed an upper respiratory tract infection. On admission, his blood pressure is 130/80 mm Hg, the heart rate 92/min, the respiratory rate 24/min, the temperature 37.6°C (99.7°F), and SaO2 on room air 87%. Chest radiograph shows consolidation in the lower lobe of the right lung. Arterial blood gases (ABG) are taken and antibiotics are started. A nasal cannula provides 2L of oxygen to the patient. When the ABG results arrive, the patient’s SaO2 is 93%. The results are as follows: pH 7.32 PaO2 63 mm Hg PaCO2 57 mm Hg HCO3- 24 mEq/L What is the most appropriate next step in the management of this patient?
A 72-year-old man comes to the physician for a routine physical examination. He says that he has felt well except for occasional headaches. He has no history of major medical illness. His temperature is 37°C (98.6°F), pulse is 80/min, and blood pressure is 155/90 mm Hg. An ultrasound of the kidneys shows a normal right kidney and a left kidney that is 2 cm smaller in length. Further evaluation is most likely to show which of the following?
A 61-year-old man presents to the office with a past medical history of hypertension, diabetes mellitus type II, hypercholesterolemia, and asthma. Recently, he describes increasing difficulty with breathing, particularly when performing manual labor. He also endorses a new cough, which occurs both indoors and out. He denies any recent tobacco use, despite a 40-pack-year history. He mentions that his symptoms are particularly stressful for him since he has been working in the construction industry for the past 30 years. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 74/min, and respiratory rate 14/min. On physical examination you notice clubbing of his digits, wheezing on auscultation, and normal heart sounds. A chest radiograph demonstrates linear opacities at the bilateral lung bases and multiple calcified pleural plaques. What is his most likely diagnosis?
A 56-year-old man who provides direct patient care on a tuberculosis ward undergoes occupational tuberculosis screening. He has no fever, night sweats, weight loss, cough, or hemoptysis. A tuberculin skin test produces 12 mm of induration, and an interferon-gamma release assay is positive. The chest radiograph shown demonstrates an approximately 2-cm spiculated nodule in the left mid-lung. CT confirms a suspicious solid left upper-lobe nodule without cavitation, tree-in-bud opacities, or other findings of active tuberculosis. The nodule is resected and found to be stage IA lung adenocarcinoma without granulomatous inflammation. Three sputum specimens obtained on separate days have negative acid-fast smears and nucleic acid amplification tests, and all three mycobacterial cultures are finalized as negative after 8 weeks. Which of the following is an appropriate preferred treatment for this patient's tuberculosis infection?

A 28-year-old woman comes to the emergency department because of increasing weakness and numbness of her legs for 3 days. She noticed that the weakness was more severe after she had a hot shower that morning. A year ago, she had an episode of partial vision loss in her left eye that resolved within 3 weeks. She is sexually active with 3 male partners and uses condoms inconsistently. She appears anxious. Her temperature is 37°C (98.6°F), pulse is 80/min, and blood pressure is 108/77 mm Hg. Examination shows spasticity and decreased muscle strength in bilateral lower extremities. Deep tendon reflexes are 4+ bilaterally. Plantar reflex shows an extensor response bilaterally. The abdominal reflex is absent. Sensation to vibration and position over the lower extremities shows no abnormalities. Tandem gait is impaired. MRI of the brain and spine is inconclusive. Further evaluation is most likely to show which of the following?
A 39-year-old woman comes to the physician because of a 5-day history of pain and stiffness in her hands and wrists and a nonpruritic generalized rash. The stiffness is worst in the morning and improves after 15–20 minutes of activity. She had fever and a runny nose 10 days ago that resolved without treatment. She is sexually active with a male partner and uses condoms inconsistently. She works as an elementary school teacher. Her temperature is 37.3°C (99.1°F), pulse is 78/min, and blood pressure is 120/70 mm Hg. Examination shows swelling, tenderness, and decreased range of motion of the wrists as well as the metacarpophalangeal and proximal interphalangeal joints. There is a lacy macular rash over the trunk and extremities. Laboratory studies, including erythrocyte sedimentation rate and anti-nuclear antibody and anti-dsDNA serology, show no abnormalities. Which of the following is the most likely cause of this patient's symptoms?
A 30-year-old woman comes to the physician because of severe headaches and lightheadedness for 2 months. She has also been hearing a 'swoosh' sound in her left ear for the past month. She has allergic rhinitis and acne. Her sister is being treated for thyroid cancer. Current medications include levocetirizine, topical clindamycin, and azelastine-fluticasone nasal spray. She appears anxious. She is 155 cm (5 ft 1 in) tall and weighs 77 kg (170 lb); BMI is 32 kg/m2. Her temperature is 37°C (98.6°F), pulse is 96/min, respirations are 14/min, and blood pressure is 168/96 mm Hg. Examination shows cystic acne over the face and back. The pupils are equal and reactive. There is a bruit on the left side of the neck. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. The abdomen is soft and nontender. There is an abdominal bruit on the left side. Neurologic examination shows no focal findings. Further evaluation of this patient is most likely to show which of the following?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app