
Cardiology — MCQs

On this page
A 49-year-old man presents to a physician with the complaint of pain in the thigh after walking. He says that he is an office clerk with a sedentary lifestyle and usually drives to his office. On 2 occasions last month he had to walk to his office, which is less than a quarter of a mile from his home. On both occasions, soon after walking, he experienced pain in the right thigh which subsided spontaneously within a few minutes. His past medical history is negative for hypertension, hypercholesterolemia, or ischemic heart disease. He is a non-smoker and non-alcoholic. His father has ischemic heart disease. His physical examination is within normal limits, and the peripheral pulses are palpable in all extremities. His detailed diagnostic evaluation, including magnetic resonance angiogram (MRA) and exercise treadmill ankle-brachial index (ABI) testing, suggests a diagnosis of peripheral vascular disease due to atherosclerosis of the right iliac artery. Which of the following is the best initial treatment option?
A 50-year-old female is evaluated by her physician for recent weight gain. Physical examination is notable for truncal obesity, wasting of her distal musculature and moon facies. In addition she complains of abnormal stretch marks that surround her abdomen. The physician suspects pituitary adenoma. Which of the following high-dose dexamethasone suppression test findings and baseline ACTH findings would support his view?
A 25-year-old man presents to the emergency department with back pain. He states that it started yesterday and has been gradually getting worse. He states that the pain is worsened with moving and lifting and is relieved with rest and ibuprofen. He has a past medical history of smoking and IV drug abuse and states he last used IV drugs 2 days ago. He thinks his symptoms may be related to lifting a heavy box. His temperature is 99.3°F (37.4°C), blood pressure is 122/88 mmHg, pulse is 77/min, respirations are 14/min, and oxygen saturation is 99% on room air. Physical exam is notable for focal back pain lateral to the patient’s spine on the left. There is no midline tenderness and the rest of the patient’s exam is unremarkable. There are scars in the antecubital fossae bilaterally. Laboratory values including a C-reactive protein are unremarkable. Which of the following is the most likely diagnosis?
A 34-year-old female presents to her primary care physician complaining of fatigue. Over the last three months she has experienced decreased energy and gained 7 pounds. Review of systems is negative for symptoms of depression but is positive for constipation, myalgias, and cold intolerance. Physical exam is notable for delayed deep tendon reflex relaxation. Vital signs are as follows: T 37.1 C, HR 61, BP 132/88, RR 16, and SpO2 100%. Which of the following is the best initial screening test for this patient?
A 63-year-old woman with a previous diagnosis of rheumatoid arthritis and Sjogren syndrome was referred for a second opinion. She has had a known chronic idiopathic pericardial effusion for about a year and has dealt with intermittent chest pain ever since. She underwent 2 diagnostic pericardiocenteses, but the fluid returned each time. She also has used empiric anti-inflammatory therapies with NSAIDs and colchicine without significant changes in the size of the pericardial effusion. The etiological testing was negative. At this visit, she is still complaining of pain in her chest but has no evidence of distended neck veins. An ECG shows sinus rhythm with low QRS voltages. What will be the procedure of choice that would be both therapeutic and diagnostic?
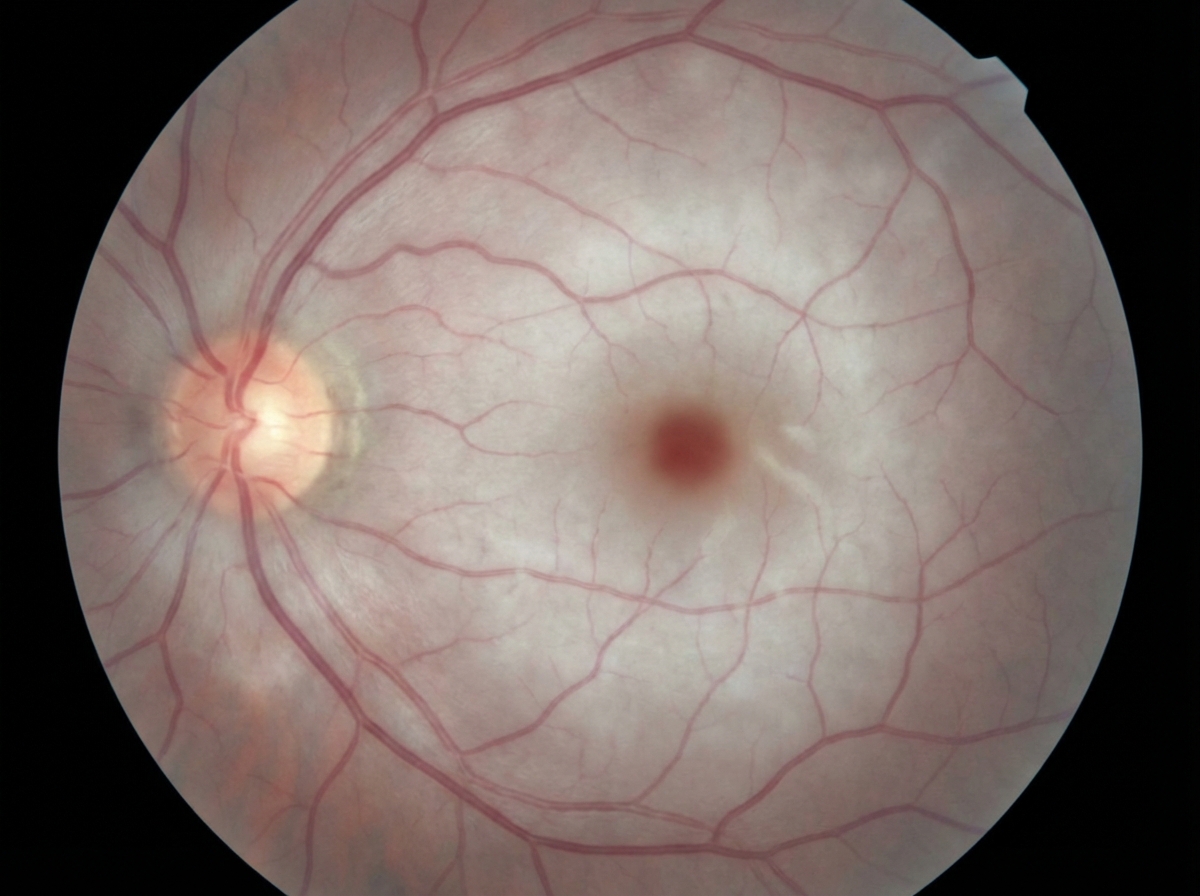
An 81-year-old man comes to the emergency department because of left-sided visual loss that started 1 hour ago. He describes initially seeing jagged edges, which was followed by abrupt, complete loss of central vision in the left eye. He has hypertension and type 2 diabetes mellitus. Blood pressure is 145/89 mm Hg. Neurologic examination shows no abnormalities. A photograph of the fundoscopic findings is shown. Which of the following tests is most likely to evaluate the likely embolic source of this patient's condition?
A 68-year-old woman is brought to the physician by her husband for the evaluation of confusion and memory deficits for the last month. During this period, she has also had mild weakness in her left leg. She has hypertension and hyperlipidemia. Her current medications include enalapril and atorvastatin. She has smoked two packs of cigarettes daily for the last 45 years. She drinks a glass of wine every day. Her temperature is 37°C (98.6°F), pulse is 75/min, and blood pressure is 135/85 mm Hg. She is oriented only to person. She recalls 2 out of 3 objects immediately and none after 5 minutes. The patient is unable to lift her eyebrows or to smile. Muscle strength is decreased in the left lower extremity. A T2-weighted MRI scan of the head shows several hyperintense round lesions in the frontal and temporal lobe at the border of the gray and white matter. Which of the following is the most likely diagnosis?
A 54-year-old man comes to the physician for an annual health maintenance examination. He reports that he feels well. He has smoked one pack of cigarettes daily for 22 years and drinks three 12-oz bottles of beer each night. He works as an accountant and says he does not have time to exercise regularly. He is 178 cm (5 ft 10 in) tall and weighs 98 kg (216 lb); BMI is 31 kg/m2. His blood pressure is 146/90 mm Hg. Physical examination shows no abnormalities. His serum cholesterol concentration is 232 mg/dL and hemoglobin A1C is 6.9%. Which of the following preventative measures is likely to have the greatest impact on this patient's all-cause mortality risk?
A 76-year-old woman comes to the physician because of increasing muscle pain and stiffness, weakness of her shoulders and legs, and generalized fatigue for the past 4 months. She has been having great difficulty getting out of bed in the morning. On two occasions her son had to come over and help her stand up. She has had a 4-kg (9-lb) weight loss and has not been sleeping well during this period. She has had multiple episodes of left-sided headaches and pain in her jaw while chewing over the past 2 months. She had a fall and hit her head on the staircase banister 3 months ago. Her temperature is 38°C (100.4°F), pulse is 101/min, and blood pressure is 128/88 mm Hg. Examination shows conjunctival pallor. Range of motion of the shoulder and hip is mildly limited by pain. Muscle strength in bilateral upper and lower extremities is normal. Deep tendon reflexes are 2+ bilaterally. On mental status examination, she admits her mood 'is not that great'. Her erythrocyte sedimentation rate is 59 mm/h and serum creatine kinase is 38 mg/dL. Which of the following is the most likely cause of this patient's headache?
A 14-year-old boy is brought to the physician because of fever, malaise, and severe right knee joint pain and swelling for 3 days. He had also had episodes of abdominal pain and epistaxis during this period. Five days ago, he had swelling and pain in his left ankle joint which has since resolved. He reports having a sore throat 3 weeks ago while he was camping in the woods, for which he received symptomatic treatment. His immunizations are up-to-date. His temperature is 38.7°C (101.6°F), pulse is 119/min, and blood pressure is 90/60 mm Hg. Examination shows a swollen, tender right knee; range of motion is limited. There are painless 3- to 4-mm nodules over the elbow. Cardiopulmonary examination is normal. His hemoglobin concentration is 12.3 g/dL, leukocyte count is 11,800/mm3, and erythrocyte sedimentation rate is 58 mm/h. Arthrocentesis of the right knee joint yields clear, straw-colored fluid; no organisms are identified on Gram stain. Analysis of the synovial fluid shows a leukocyte count of 1,350/mm3 with 17% neutrophils. Which of the following is the most likely diagnosis?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app