
Cardiology — MCQs

On this page
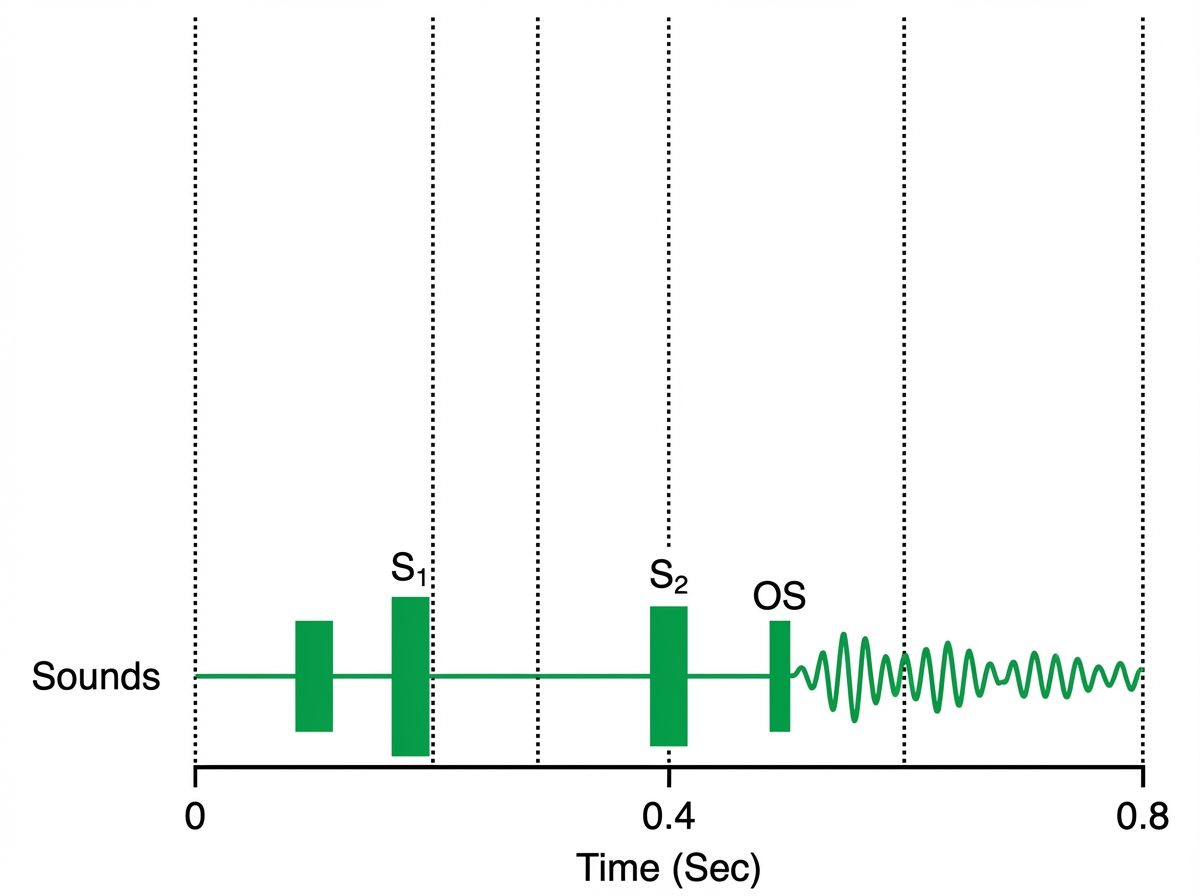
A 45-year-old woman comes to the physician because of shortness of breath while lying on her back over the past month. During this period, she has also had several episodes of bloody coughing. The patient reports that she had a heart problem when she was a child that was treated with antibiotics. She emigrated to the US from Russia 5 years ago. There is no family history of serious illness. Pulmonary examination shows crackles at both lung bases. Cardiac examination is shown. An ECG shows tachycardia and no P waves. Which of the following is the most likely diagnosis?
A previously healthy 48-year-old man comes to the physician for a 3-month history of myalgias and recurrent episodes of retrosternal chest pain and dizziness. He has had a 5-kg (11-lb) weight loss during this period. His temperature is 39.1°C (102.3°F), pulse is 90/min, and blood pressure is 160/102 mm Hg. Physical examination shows lacy, purplish discoloration of the skin with multiple erythematous, tender subcutaneous nodules on the lower legs. Some of the nodules have central ulcerations. Serum studies show an erythrocyte sedimentation rate of 76 mg/dL and creatinine level of 1.8 mg/dL. Renal MR angiography shows irregular areas of dilation and constriction in the renal arteries bilaterally. Further evaluation of this patient is most likely to show which of the following?
A previously healthy 35-year-old woman comes to the emergency department because of a sudden onset of difficulty breathing that began when she woke up that morning. She also reports a dry cough and chest pain that is worse with inspiration. She does not smoke, drink alcohol, or use illicit drugs. Her only medication is an oral contraceptive. Her temperature is 38°C (100.4°F), pulse is 90/min, respirations are 22/min, and blood pressure is 120/70 mm Hg. Oxygen saturation is 93% on room air. Physical examination is unremarkable. An ECG shows non-specific ST segment changes. An x-ray of the chest shows no abnormalities. In addition to oxygen supplementation, which of the following is the most appropriate next step in management?
A 12-year-old boy presents with a 3-day history of frothy brown urine. He does not complain of any other symptoms. He notes that 3 weeks ago he had a fever with a sore throat, but he did not receive any treatment at the time. His blood pressure is 152/94 mm Hg, heart rate is 72/min, respiratory rate is 15/min, and temperature is 37.0°C (98.6°F). Review of his medical record shows that his blood pressure was 118/74 mm Hg just 4 weeks ago. Laboratory analysis reveals elevated serum creatinine, hematuria with RBC casts, and elevated urine protein without frank proteinuria. What laboratory test can confirm the most likely diagnosis in this patient?
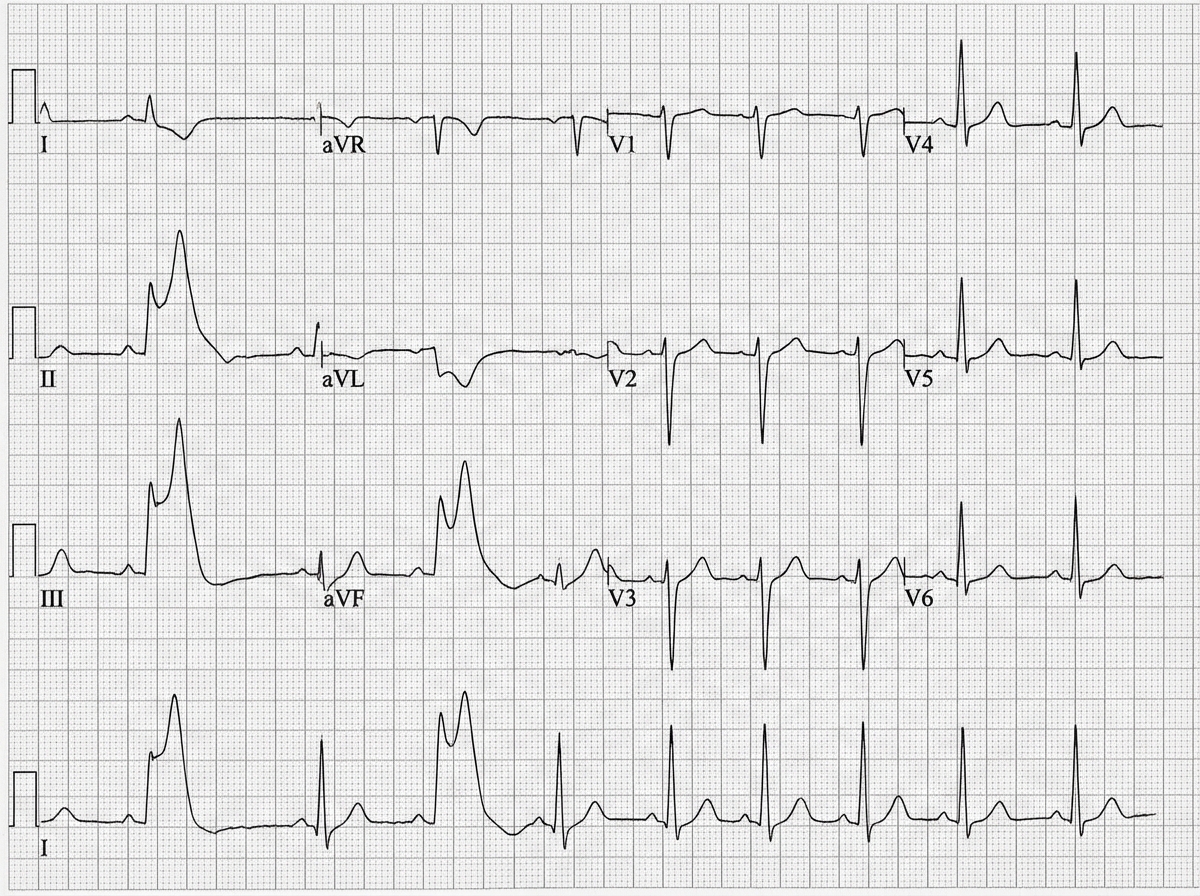
A 64-year-old woman comes to the physician because of worsening intermittent nausea and burning pain in her upper abdomen for 4 hours. She has not had retrosternal chest pain, shortness of breathing, or vomiting. She has hypertension and type 2 diabetes mellitus. She has smoked one pack of cigarettes daily for 20 years. Her only medications are lisinopril and insulin. Her temperature is 37°C (98.6°F), pulse is 90/min, respirations are 12/min, and blood pressure is 155/75 mm Hg. The lungs are clear to auscultation. The abdomen is soft, with mild tenderness to palpation of the epigastrium but no guarding or rebound. Bowel sounds are normal. An ECG is shown. This patient's current condition is most likely to cause which of the following findings on cardiac examination?
A 78-year-old male has been hospitalized for the past 3 days after undergoing a revision left total hip replacement. Over the past several hours, the nursing staff reports that the patient has exhibited fluctuating periods of intermittent drowsiness and confusion where he has been speaking to nonexistent visitors in his hospital room. The patient's daughter is present at bedside and reports that the patient lives alone and successfully manages his own affairs without assistance. Which of the following is most likely true of this patient's current condition?
Eight hours after undergoing successful cholecystectomy, a 65-year-old man with scoliosis complains of shortness of breath. Respirations are 28/min and pulse oximetry on room air shows an oxygen saturation of 85%. Physical examination shows kyphotic deformation of the thorax. Cardiopulmonary examination shows intercostal retractions and diminished breath sounds on the left side. There is trace pedal edema bilaterally. An x-ray of the chest shows bilateral fluffy infiltrates, and the cardiac silhouette is shifted slightly to the left side. Which of the following is the most likely explanation for this patient's hypoxia?
A 27-year-old male basketball player presents to his primary care physician for a normal check-up. He has not been seen by a physician in ten years. He reports that he feels well and has no complaints. His temperature is 98.6°F (37°C), blood pressure is 110/70 mmHg, pulse is 85/min, and respirations are 16/min. On examination, the patient's height is 76 in (193 cm) with an arm span of 78 in (198 cm). His BMI is 19 kg/m^2. His fingers and toes are long and tapered and his sternum appears sunken into his chest. The patient also has moderate scoliosis. Upon further questioning, the patient reports that his father had a similar physique but passed away in his 40s. Which of the following complications is this patient at greatest risk for?
An 18-year-old man is brought to the emergency department due to the confusion that started earlier in the day. His parents report that the patient had recovered from vomiting and diarrhea 3 days ago without medical intervention. They mention that although nausea and vomiting have resolved, the patient continued to have diffuse abdominal pain and decreased appetite. Past medical history is unremarkable, except for a recent weight loss and increased thirst. The patient does not use tobacco products or alcohol. He is not sexually active and does not use illicit drugs. He appears lethargic but responds to questions. His mucous membranes appear dry. Temperature is 36.9°C (98.4°F), blood pressure is 105/60 mm Hg, pulse is 110/min, and respiratory rate is 27/min with deep and rapid respiration. There is diffuse abdominal tenderness without guarding, rebound tenderness or rigidity. Which of the following is the next best step in the management of this patient?
A 34-year-old man comes to the physician because of increasing lower back and neck pain for the past 7 months. The pain is worse in the morning and improves when he plays basketball. He has noticed shortness of breath while playing for the past 2 months. He is sexually active with 2 female partners and uses condoms inconsistently. He appears lethargic. His vital signs are within normal limits. Examination of the back shows tenderness over the sacroiliac joints. Range of motion is limited. The lungs are clear to auscultation. Chest expansion is decreased on full inspiration. His leukocyte count is 14,000/mm3 and erythrocyte sedimentation rate is 84 mm/h. An x-ray of the spine shows erosion and sclerosis of the sacroiliac joints and loss of spinal lordosis. Further evaluation of this patient is most likely to show which of the following?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app