
Cardiology — MCQs

On this page
A 37-year-old woman presents to the emergency department complaining of generalized malaise, weakness, headache, nausea, vomiting, and diarrhea; she last felt well roughly two days ago. She is otherwise healthy, and takes no medications. Her vital signs are: T 38.0, HR 96 beats per minute, BP 110/73, and O2 sat 96% on room air. Examination reveals a somewhat ill-appearing woman; she is drowsy but arousable and has no focal neurological deficits. Initial laboratory studies are notable for hematocrit 26%, platelets of 80,000/mL, and serum creatinine of 1.5 mg/dL. Which of the following is the most appropriate treatment at this time?
A 60-year-old man comes to the physician for an examination prior to a scheduled cholecystectomy. He has hypertension treated with hydrochlorothiazide. His mother had chronic granulomatous disease of the lung. He works in a glass manufacturing plant. He has smoked two packs of cigarettes daily for 38 years. His vital signs are within normal limits. Examination shows no abnormalities. Laboratory studies are within the reference range. An x-ray of the chest is shown. Which of the following is the most appropriate next step in management?

A 60-year-old man seeks evaluation at a medical office due to leg pain while walking. He says the pain starts in his buttocks and extends to his thighs and down to his calves. Previously, the pain resolved with rest, but the pain now persists in his feet, even during rest. His past medical history is significant for diabetes mellitus, hypertension, and cigarette smoking. The vital signs are within normal limits. The physical examination shows an atrophied leg with bilateral loss of hair. Which of the following is the most likely cause of this patient’s condition?
A 35-year-old woman comes to the physician because of a 1-month history of double vision, difficulty climbing stairs, and weakness when trying to brush her hair. She reports that these symptoms are worse after she exercises and disappear after she rests for a few hours. Physical examination shows drooping of her right upper eyelid that worsens when the patient is asked to gaze at the ceiling for 2 minutes. There is diminished motor strength in the upper extremities. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?
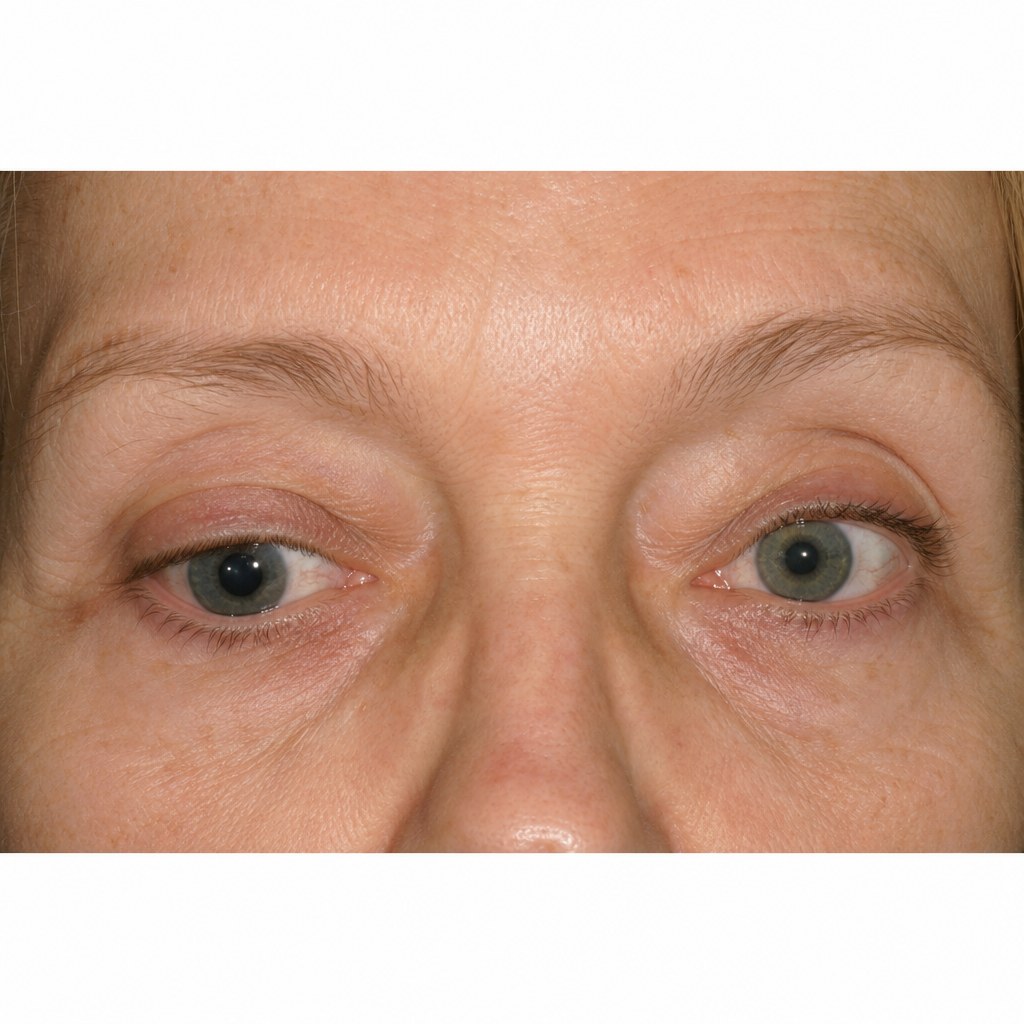
A 63-year-old woman presents to her primary-care doctor for a 2-month history of vision changes, specifically citing the gradual onset of double vision. Her double vision is present all the time and does not get better or worse throughout the day. She has also noticed that she has a hard time keeping her right eye open, and her right eyelid looks 'droopy' in the mirror. Physical exam findings during primary gaze are shown in the photo. Her right pupil is 6 mm and poorly reactive to light. The rest of her neurologic exam is unremarkable. Laboratory studies show an Hb A1c of 5.0%. Which of the following is the next best test for this patient?
A 53-year-old man comes to the emergency department because of severe right-sided flank pain for 3 hours. The pain is colicky, radiates towards his right groin, and he describes it as 8/10 in intensity. He has vomited once. He has no history of similar episodes in the past. Last year, he was treated with naproxen for swelling and pain of his right toe. He has a history of hypertension. He drinks one to two beers on the weekends. Current medications include amlodipine. He appears uncomfortable. His temperature is 37.1°C (99.3°F), pulse is 101/min, and blood pressure is 130/90 mm Hg. Examination shows a soft, nontender abdomen and right costovertebral angle tenderness. An upright x-ray of the abdomen shows no abnormalities. A CT scan of the abdomen and pelvis shows a 7-mm stone in the proximal ureter and grade I hydronephrosis on the right. Which of the following is most likely to be seen on urinalysis?
A 69-year-old male presents to the emergency room with back pain. He has a history of personality disorder and metastatic prostate cancer and was not a candidate for surgical resection. He began chemotherapy but discontinued due to unremitting nausea. He denies any bowel or bladder incontinence. He has never had pain like this before and is demanding morphine. The nurse administers IV morphine and he feels more comfortable. Vital signs are stable. On physical examination you note tenderness to palpation along the lower spine, weakness in the bilateral lower extremities, left greater than right. Neurological examination is also notable for hyporeflexia in the knee and ankle jerks bilaterally. You conduct a rectal examination, which reveals saddle anesthesia. Regarding this patient, what is the most likely diagnosis and the appropriate next step in management?
A 68-year-old man comes to the physician because of recurrent episodes of nausea and abdominal discomfort for the past 4 months. The discomfort is located in the upper abdomen and sometimes occurs after eating, especially after a big meal. He has tried to go for a walk after dinner to help with digestion, but his complaints have only increased. For the past 3 weeks he has also had symptoms while climbing the stairs to his apartment. He has type 2 diabetes mellitus, hypertension, and stage 2 peripheral arterial disease. He has smoked one pack of cigarettes daily for the past 45 years. He drinks one to two beers daily and occasionally more on weekends. His current medications include metformin, enalapril, and aspirin. He is 168 cm (5 ft 6 in) tall and weighs 126 kg (278 lb); BMI is 45 kg/m2. His temperature is 36.4°C (97.5°F), pulse is 78/min, and blood pressure is 148/86 mm Hg. On physical examination, the abdomen is soft and nontender with no organomegaly. Foot pulses are absent bilaterally. An ECG shows no abnormalities. Which of the following is the most appropriate next step in diagnosis?
A 46-year-old woman comes to the physician because of a 2-week history of diplopia and ocular pain when reading the newspaper. She also has a 3-month history of amenorrhea, hot flashes, and increased sweating. She reports that she has been overweight all her adult life and is happy to have lost 6.8-kg (15-lb) of weight in the past 2 months. Her pulse is 110/min, and blood pressure is 148/98 mm Hg. Physical examination shows moist palms and a nontender thyroid gland that is enlarged to two times its normal size. Ophthalmologic examination shows prominence of the globes of the eyes, bilateral lid retraction, conjunctival injection, and an inability to converge the eyes. There is no pain on movement of the extraocular muscles. Visual acuity is 20/20 bilaterally. Neurologic examination shows a fine resting tremor of the hands. Deep tendon reflexes are 3+ with a shortened relaxation phase. Which of the following is the most likely cause of this patient's ocular complaints?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app