
Cardiology — MCQs

On this page
A 72-year-old man presents to his primary care provider complaining of fatigue, mild headache, and discomfort with chewing for roughly 1 week. Before this, he felt well overall, but now he is quite bothered by these symptoms. His medical history is notable for hypertension and hyperlipidemia, both controlled. On examination, he is uncomfortable but nontoxic-appearing. There is mild tenderness to palpation over his right temporal artery, but otherwise the exam is not revealing. Prompt recognition and treatment can prevent which of the following feared complications:
A 29-year-old female presents to her primary care provider complaining of pain and stiffness in her hands and knees. She reports that the stiffness is worse in the morning and appears to get better throughout the day. She is otherwise healthy and denies any recent illness. She does not play sports. On examination, her metacarpal-phalangeal (MCP) and proximal interphalangeal (PIP) joints are swollen and erythematous. Her distal interphalangeal (DIP) joints appear normal. She exhibits pain with both passive and active range of motion in her knees bilaterally. Serological analysis reveals high titers of anti-cyclic citrullinated peptide antibodies. Which of the following processes underlies this patient’s condition?
A 49-year-old man comes to the physician because of a 6-month history of increasing fatigue and reduced libido. He also complains of joint pain in both of his hands. His vital signs are within normal limits. Physical examination shows tanned skin and small testes. The second and third metacarpophalangeal joints of both hands are tender to palpation and range of motion is limited. The liver is palpated 2 to 3 cm below the right costal margin. Histopathologic examination of a liver biopsy specimen shows intracellular material that stains with Prussian blue. This patient is at greatest risk for developing which of the following complications?
A 6-year-old boy is brought to the emergency room by ambulance, accompanied by his kindergarten teacher. Emergency department staff attempt to call his parents, but they cannot be reached. The boy’s medical history is unknown. According to his teacher, the boy was eating in the cafeteria with friends when he suddenly complained of itching and developed a widespread rash. Physical exam is notable for diffuse hives and tongue edema. His pulse is 100/min and blood pressure is 90/60 mmHg. The boy appears frightened and tells you that he does not want any treatment until his parents arrive. Which of the following is the next best step in the management of this patient?
A 23-year-old woman is brought to the emergency department 8 hours after the sudden onset of shortness of breath and pleuritic chest pain. She has cystic fibrosis and, during the past year, has had 4 respiratory exacerbations that have required hospitalization. Current medications include an inhaled bronchodilator, an inhaled corticosteroid, inhaled N-acetylcysteine, and azithromycin. The patient appears chronically ill. Her temperature is 37.9°C (100.2°F), pulse is 96/min, respirations are 22/min and labored, and blood pressure is 106/64 mm Hg. Pulse oximetry on 2 L/min of oxygen via nasal cannula shows an oxygen saturation of 96%. Examination shows an increased anteroposterior chest diameter. There is digital clubbing. Chest excursions and tactile fremitus are decreased on the right side. On auscultation of the chest, breath sounds are significantly diminished over the right lung field and diffuse wheezing is heard over the left lung field. Which of the following is the most likely underlying cause of this patient's current symptoms?
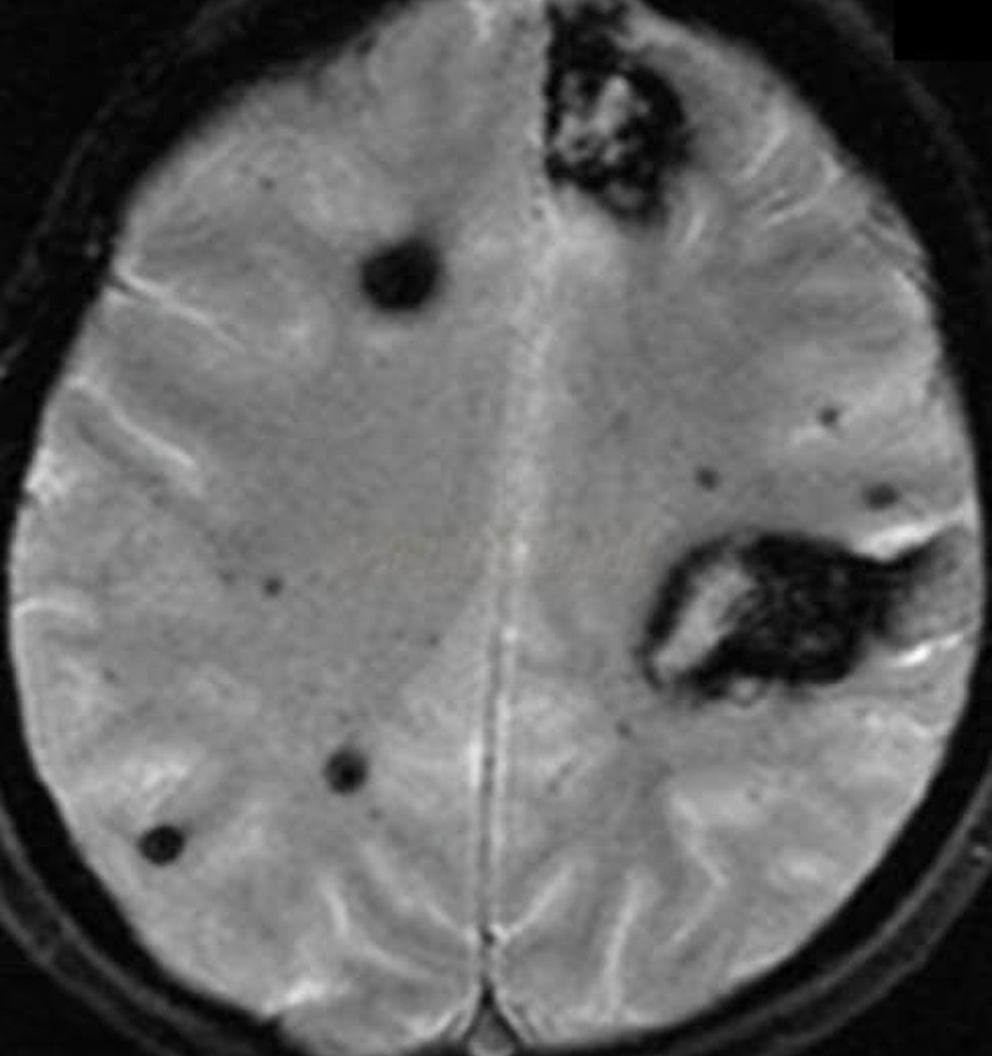
An 88-year-old woman with no significant medical history is brought to the emergency room by her daughter after a fall, where the woman lightly hit her head against a wall. The patient is lucid and complains of a mild headache. The daughter indicates that her mother did not lose consciousness after the fall. On exam, there are no focal neurological deficits, but you decide to perform a CT scan to be sure there is no intracranial bleeding. The CT scan is within normal limits and head MRI is performed (shown). Which of the following conditions has the most similar risk factor to this patient's condition?
A 60-year-old male presents for a routine health check-up. The patient complains of reduced exercise tolerance for the past 2 years. Also, in the past year, he has noticed chest pain after climbing the stairs in his home. He has no significant past medical history or current medications. The patient reports a 45-pack-year smoking history. The vital signs include temperature 37.0°C (98.6°F), blood pressure 160/100 mm Hg, pulse 72/min, respiratory rate 15/min, and oxygen saturation 99% on room air. His body mass index (BMI) is 34 kg/m2. Physical examination is unremarkable. Laboratory studies show: Serum total cholesterol 265 mg/dL HDL 22 mg/dL LDL 130 mg/dL Triglycerides 175 mg/dL HDL: high-density lipoprotein; LDL: low-density lipoprotein Which of the following vascular pathologies is most likely present in this patient?
A 58-year-old man presents to the emergency department for evaluation of intermittent chest pain over the past 6 months. His history reveals that he has had moderate exertional dyspnea and 2 episodes of syncope while working at his factory job. These episodes of syncope were witnessed by others and lasted roughly 30 seconds. The patient states that he did not have any seizure activity. His vital signs include: blood pressure 121/89 mm Hg, heart rate 89/min, temperature 37.0°C (98.6°F), and respiratory rate 16/min. Physical examination reveals a crescendo-decrescendo systolic murmur in the right second intercostal area. An electrocardiogram is performed, which shows left ventricular hypertrophy. Which of the following is the best next step for this patient?
An 82-year-old comes to the physician for a routine checkup. He feels well. He has a history of hypertension, peripheral vascular disease, carotid stenosis, and mild dementia. His father had Parkinson's disease and died of a stroke at the age of 74 years. He has smoked one-half pack of cigarettes daily for 30 years but quit at the age of 50 years. He drinks alcohol in moderation. Current medications include aspirin and lisinopril. He appears healthy. His temperature is 36.9°C (98.4°F), pulse is 73/min, respirations are 12/min, and blood pressure is 142/92 mmHg. Examination shows decreased pedal pulses bilaterally. Ankle jerk and patellar reflexes are absent bilaterally. Sensation to light touch, pinprick, and proprioception is intact bilaterally. Muscle strength is 5/5 bilaterally. He describes the town he grew up in with detail but only recalls one of three words after 5 minutes. Which of the following is the most appropriate next step in management for these findings?
A 48-year-old female complains of tingling sensation in her fingertips as well as the skin around her mouth which woke her up from sleep. She is in the postoperative floor as she just underwent a complete thyroidectomy for papillary thyroid cancer. Her temperature is 37° C (98.6° F), respirations are 15/min, pulse is 67/min, and blood pressure is 122/88 mm Hg. While recording the blood pressure, spasm of the muscles of the hand and forearm is seen. What is the next best step in the management of this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app