
Cardiology — MCQs

On this page
A 55-year-old woman presents to her primary care provider with a 2-month history of insidious onset of left shoulder pain. It only occurs at the extremes of her range of motion and has made it difficult to sleep on the affected side. She has noticed increasing difficulty with activities of daily living, including brushing her hair and putting on or taking off her blouse and bra. She denies a history of shoulder trauma, neck pain, arm/hand weakness, numbness, or paresthesias. Her medical history is remarkable for type 2 diabetes mellitus, for which she takes metformin and glipizide. Her physical examination reveals a marked decrease in both active and passive range of motion of the left shoulder, with forwarding flexion to 75°, abduction to 75°, external rotation to 45°, and internal rotation to 15° with significant pain. Rotator cuff strength is normal. AP, scapular Y, and axillary plain film radiographs are reported as normal. Which of the following is the most likely diagnosis?
A 48-year-old female presents to the emergency room with mental status changes. Laboratory analysis of the patient's serum shows: Na 122 mEq/L K 3.9 mEq/L HCO3 24 mEq/L BUN 21 mg/dL Cr 0.9 mg/dL Ca 8.5 mg/dL Glu 105 mg/dL Urinalysis shows: Osmolality 334 mOsm/kg Na 45 mEq/L Glu 0 mg/dL Which of the following is the most likely diagnosis?
An 11-year-old boy presents with fever and joint pain for the last 3 days. His mother says that he had a sore throat 3 weeks ago but did not seek medical care at that time. The family immigrated from the Middle East 3 years ago. The patient has no past medical history. The current illness started with a fever and a swollen right knee that was very painful. The following day, his knee improved but his left elbow became swollen and painful. While in the waiting room, his left knee is also becoming swollen and painful. Vital signs include: temperature 38.7°C (101.6°F), and blood pressure 110/80 mm Hg. On physical examination, the affected joints are swollen and very tender to touch, and there are circular areas of redness on his back and left forearm (as shown in the image). Which of the following is needed to establish a diagnosis of acute rheumatic fever in this patient?

A 52-year-old woman presents to her primary care physician with a chief complaint of diarrhea. She states that it has been going on for the past month and started after she ate a burger cooked over a campfire. She endorses having lost 10 pounds during this time. The patient has no other complaints other than hoarseness which has persisted during this time. The patient has a past medical history of obesity, hypothyroidism, diabetes, and anxiety. Her current medications include insulin, metformin, levothyroxine, and fluoxetine. She currently drinks 4 to 5 alcoholic beverages per day. Her temperature is 99.5°F (37.5°C), blood pressure is 157/98 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. On physical exam, you note a healthy obese woman. Cardiopulmonary exam is within normal limits. HEENT exam is notable for a mass on the thyroid. Abdominal exam is notable for a candida infection underneath the patient's pannus. Pelvic exam is notable for a white, fish-odored discharge. Laboratory values are as follows: Hemoglobin: 12 g/dL Hematocrit: 36% Leukocyte count: 4,500 cells/mm^3 with normal differential Platelet count: 190,000/mm^3 Serum: Na+: 141 mEq/L Cl-: 102 mEq/L K+: 5.5 mEq/L HCO3-: 24 mEq/L Glucose: 122 mg/dL Ca2+: 7.1 mg/dL Which of the following could also be found in this patient?
A 28-year-old male presents with sharp, stabbing chest pain that worsens when lying flat and improves when sitting forward. He reports a recent viral upper respiratory infection 2 weeks ago. On examination, a friction rub is heard on auscultation. His vital signs are stable. An ECG is most likely to show which of the following findings in this patient?
An 82-year-old woman is brought to the emergency department after losing consciousness at her nursing home. She had been watching TV for several hours and while getting up to use the bathroom, she fell and was unconscious for several seconds. She felt dizzy shortly before the fall. She does not have a headache or any other pain. She has a history of hypertension, intermittent atrial fibrillation, and stable angina pectoris. Current medications include warfarin, aspirin, hydrochlorothiazide, and a nitroglycerin spray as needed. Her temperature is 36.7°C (98.1°F), pulse is 100/min and regular, and blood pressure is 102/56 mm Hg. Physical exam shows a dry tongue. A fold of skin that is pinched on the back of her hand unfolds after 2 seconds. Cardiopulmonary examination shows no abnormalities. Further evaluation of this patient is most likely to show which of the following findings?
A 24-year-old man presents to his primary care physician for a persistent and low grade headache as well as trouble focusing. The patient was seen in the emergency department 3 days ago after hitting his head on a branch while biking under the influence of alcohol. His head CT at the time was normal, and the patient was sent home with follow up instructions. Since the event, he has experienced trouble focusing on his school work and feels confused at times while listening to lectures. He states that he can’t remember the lectures and also says he has experienced a sensation of vertigo at times. On review of systems, he states that he has felt depressed lately and has had trouble sleeping, though he denies any suicidal or homicidal ideation. His temperature is 98.2°F (36.8°C), blood pressure is 122/65 mmHg, pulse is 70/min, respirations are 12/min, and oxygen saturation is 98% on room air. The patient’s neurological and cardiopulmonary exam are within normal limits. Which of the following is the best next step in management?
A 29-year-old African American female presents to your office with extreme fatigue and bilateral joint pain. Serologies demonstrate the presence of rheumatoid factor along with anti-Smith and anti-dsDNA antibodies. A VDRL syphilis test is positive. You order a coagulation profile, which reveals normal bleeding time, normal PT, and prolonged PTT as well as normal platelet count. Further evaluation is most likely to reveal which of the following?
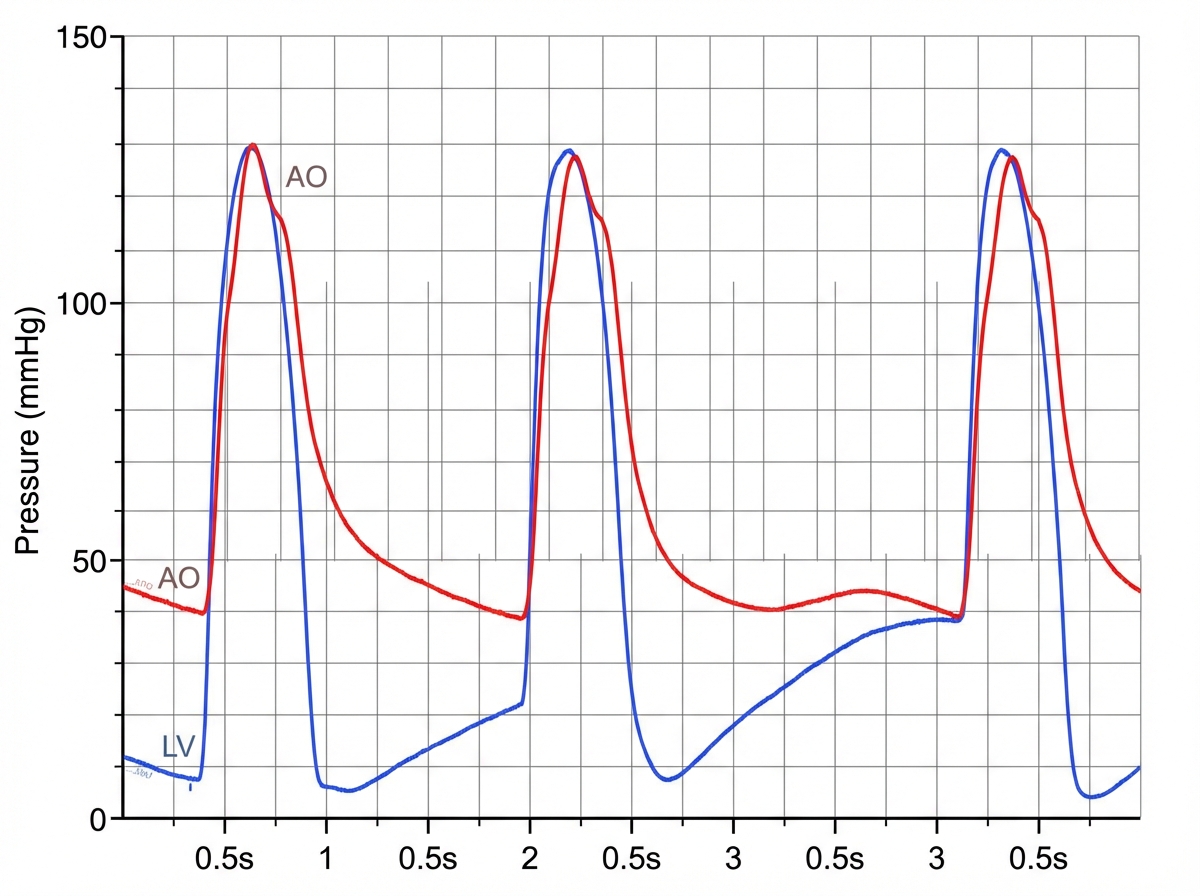
A 31-year-old man comes to the physician because of a 5-day history of fever, chills, and dyspnea. His temperature is 38.9°C (102°F) and pulse is 90/min. Cardiac examination shows a murmur. In addition to other measures, cardiac catheterization is performed. A graph showing the results of the catheterization is shown. This patient most likely has which of the following valvular heart defects?
A 52-year-old woman comes to the physician because of a 4-month history of progressive pain and stiffness of the fingers of her right hand that is worse at the end of the day. She works as a hair dresser and has to take frequent breaks to rest her hand. She has hypertension, for which she takes hydrochlorothiazide. Two weeks ago, she completed a course of oral antibiotics for a urinary tract infection. Her sister has systemic lupus erythematosus. She drinks one to two beers daily and occasionally more on weekends. Over the past 2 weeks, she has been taking ibuprofen as needed for the joint pain. Her vital signs are within normal limits. Physical examination shows swelling, joint-line tenderness, and decreased range of motion of the right first metacarpophalangeal joint as well as the 2nd and 4th distal interphalangeal joints of the right hand. Discrete, hard, mildly tender swellings are palpated over the 2nd and 4th distal interphalangeal joints of the right hand. Which of the following is the most likely underlying mechanism for these findings?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app