
Cardiology — MCQs

On this page
A 55-year-old man with no significant medical history returns for follow-up of a fasting blood glucose (FBG) of 110 mg/dL. His mother had a myocardial infarction at age 52. He weighs 90 kg and his body mass index is 35 kg/m2. His repeat FBG is 160 mg/dL and hemoglobin A1c (HbA1c) is 7.0%. He is started on metformin but is lost to follow-up. Two years later, his HbA1c is 7.6% despite maximal metformin usage, so the patient is started on glyburide. Three months later, his HbA1c is 7.3% while on both medications, and subsequently prescribed glargine and aspart. Three months later, he is brought by his wife to the emergency department for evaluation of altered mental status. His electronic medical record notes that he was started on nitrofurantoin recently for a urinary tract infection. He is disoriented to place and time. His temperature is 99°F (37.2°C), blood pressure is 90/60 mmHg, pulse is 130/min, respirations are 26/min. His basic metabolic panel is shown below: Serum: Na+: 119 mEq/L Cl-: 90 mEq/L K+: 4.2 mEq/L HCO3-: 24 mEq/L BUN: 25 mg/dL Glucose: 1,400 mg/dL Creatinine: 1.9 mg/dL His urine dipstick is negative for ketones. A peripheral intravenous line is established. What is the best initial step in management?
A 70-year-old man presented to a medical clinic for a routine follow-up. He has had hypertension for 20 years and is currently on multiple anti-hypertensive medications. The blood pressure is 150/100 mm Hg. The remainder of the examinations were within normal limits. Echocardiography showed some changes in the left ventricle. What is the most likely reason for the change?
A 14-year-old male presents to the emergency department with altered mental status. His friends who accompanied him said that he complained of abdominal pain while camping. They denied his consumption of anything unusual from the wilderness, or any vomiting or diarrhea. His temperature is 100.5°F (38.1°C), blood pressure is 95/55 mmHg, pulse is 130/min, and respirations are 30/min. His pupils are equal and reactive to light bilaterally. The remainder of the physical exam is unremarkable. His basic metabolic panel is displayed below: Serum: Na+: 116 mEq/L Cl-: 70 mEq/L K+: 4.0 mEq/L HCO3-: 2 mEq/L BUN: 50 mg/dL Glucose: 1010 mg/dL Creatinine: 1.2 mg/dL While the remainder of his labs are pending, the patient becomes bradypneic and is intubated. His ventilator is adjusted to volume control assist-control with a respiratory rate (RR) of 14/min, tidal volume (Vt) of 350 mL, positive end-expiratory pressure (PEEP) of 5 cm H2O, and fractional inspired oxygen (FiO2) of 40%. His height is 5 feet 5 inches. Intravenous fluids and additional medical therapy are administered. An arterial blood gas obtained after 30 minutes on these settings shows the following: pH: 7.05 pCO2 :40 mmHg pO2: 150 mmHg SaO2: 98% What is the best next step in management?
A 65-year-old man presents to the emergency department for sudden weakness. The patient states that he was at home enjoying his morning coffee when his symptoms began. He says that his left arm suddenly felt very odd and weak thus prompting him to come to the ED. The patient has a past medical history of diabetes, COPD, hypertension, anxiety, alcohol abuse, and PTSD. He recently fell off a horse while horseback riding but claims to not have experienced any significant injuries. He typically drinks 5-7 drinks per day and his last drink was yesterday afternoon. His current medications include insulin, metformin, atorvastatin, lisinopril, albuterol, and fluoxetine. His temperature is 99.5°F (37.5°C), blood pressure is 177/118 mmHg, pulse is 120/min, respirations are 18/min, and oxygen saturation is 93% on room air. On physical exam, you note an elderly man who is mildly confused. Cardiopulmonary exam demonstrates bilateral expiratory wheezes and a systolic murmur along the right upper sternal border that radiates to the carotids. Neurological exam reveals cranial nerves II-XII as grossly intact with finger-nose exam mildly abnormal on the left and heel-shin exam within normal limits. The patient has 5/5 strength in his right arm and 3/5 strength in his left arm. The patient struggles to manipulate objects such as a pen with his left hand. The patient is given a dose of diazepam and started on IV fluids. Which of the following is the most likely diagnosis in this patient?
A 40-year-old woman with a past medical history significant for pernicious anemia and vitiligo presents to the physician with the chief complaints of heat intolerance and frequent palpitations. The patient does not take birth control and her urine pregnancy test is negative today. Physical exam reveals a patient that is hyper-reflexive with a non-tender symmetrically enlarged thyroid gland. You order thyroid function tests for workup. What thyroid function values are most expected?
A 25-year-old man is brought to the physician because of fatigue, lethargy, and lower leg swelling for 2 weeks. He also noticed that his urine appeared darker than usual and for the last 2 days he has passed only small amounts of urine. His temperature is 37.5°C (98.6°F), pulse is 88/min, respirations are 15/min, and blood pressure is 154/98 mm Hg. Examination shows 2+ pretibial edema bilaterally. Laboratory studies show: Hemoglobin 10.9 g/dL Leukocyte count 8200/mm3 Platelet count 220,000/mm3 Serum Na+ 137 mEq/L Cl- 102 mEq/L K+ 4.8 mEq/L HCO3- 22 mEq/L Glucose 85 mg/dL Urea nitrogen 34 mg/dL Creatinine 1.4 mg/dL Urine Blood 2+ Protein 3+ Glucose negative RBC 10–12/HPF with dysmorphic features RBC casts numerous Renal biopsy specimen shows a crescent formation in the glomeruli with extracapillary cell proliferation. Which of the following is the most appropriate next step in management?
A 58-year-old woman is brought to the emergency department for shortness of breath and chest pain. Pulmonary angiography shows a large saddle embolus in the pulmonary arteries. Emergency drug therapy is administered and she is admitted to the hospital for observation. A follow-up CT scan of the chest shortly after admission shows that the thrombus has disappeared. Five hours later, the patient is found to be lethargic with slurred speech. Physical examination shows decreased consciousness, dysarthria, and optic disc swelling bilaterally. Which of the following is the most likely cause of her neurological symptoms?
A 67-year-old man comes to the office due to pain in the lower part of his calves on his afternoon walk to get the mail. The pain is relieved by rest. It started slowly about 6 months ago and has become more painful over time. He has a history of hypertension, hyperlipidemia, diabetes mellitus, and a 20-pack-year smoking history. Medications include hydrochlorothiazide, atorvastatin, metformin, and a multivitamin that he takes daily. The patient quit smoking 2 years ago and only drinks socially. Today, his blood pressure is 145/90 mm Hg, pulse is 75/min, respiratory rate is 17/min, and temperature is 37.6°C (99.6°F). On physical exam, he appears mildly obese and healthy. His heart has a regular rate and rhythm, and his lungs are clear to auscultation bilaterally. Examination of the legs shows atrophic changes and diminished pedal pulses. A measure of his ankle brachial index (ABI) is 0.89. Which of the following is the most appropriate initial treatment?
A 51-year-old female presents to her primary care physician complaining of body aches and constipation. She reports that her "bones hurt" and that she has experienced worsening constipation over the past few months. Her medical history is notable for three kidney stones within the past year that both passed spontaneously. Her vital signs are stable. Physical examination reveals a small nodule near the right inferior pole of the thyroid, consistent with a parathyroid adenoma. Which of the following sets of serum findings is most likely in this patient?
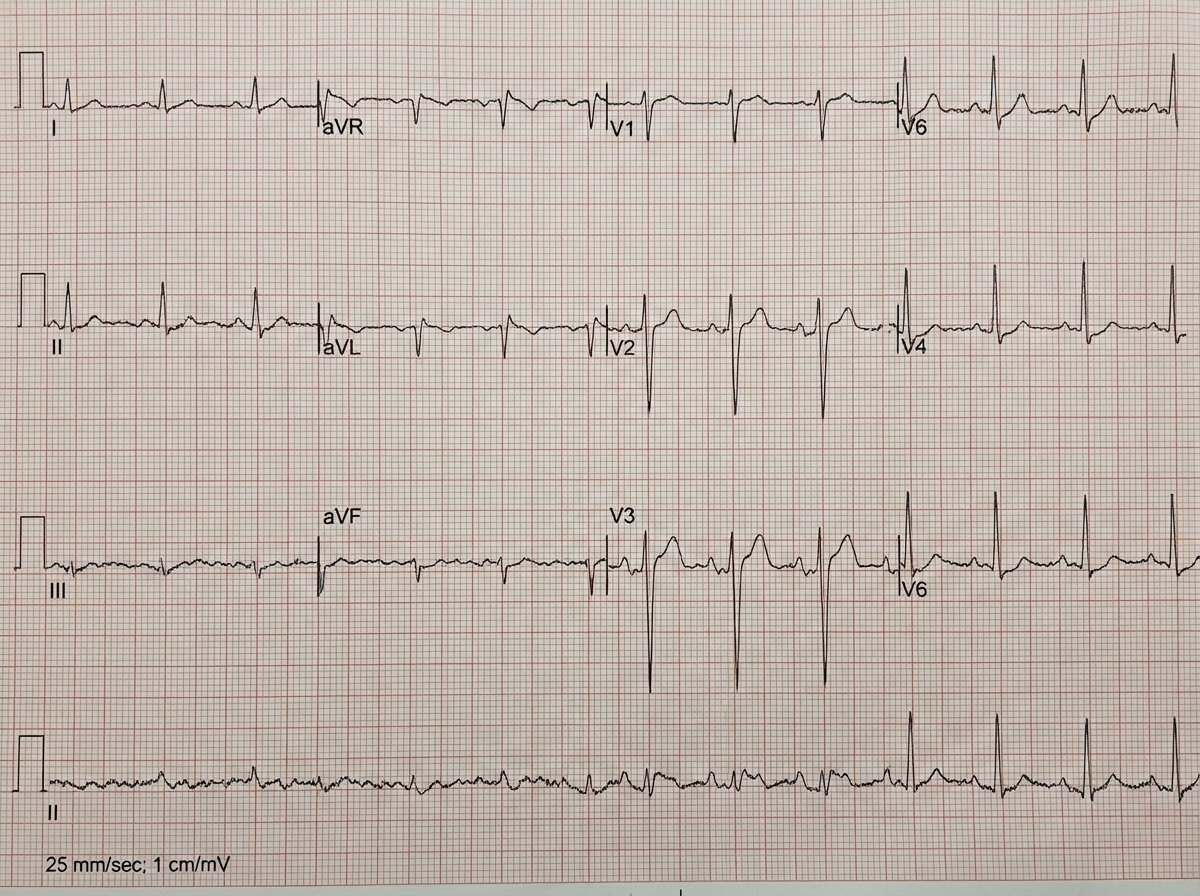
An 81-year-old woman comes to the emergency department due to a right-sided paralysis for the past 2 hours. Her husband says her symptoms began suddenly, and she is also unable to speak. Her pulse is 90/min, respirations are 18/min, temperature is 36.8°C (98.2°F), and blood pressure is 150/98 mm Hg. An ECG is obtained and is shown below. Which of the following is the most probable cause of the patient's paralysis?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app