
Cardiology — MCQs

On this page
A 42-year-old woman presents to her family physician with a headache. The patient reports that the symptoms started about 2 hours ago when she woke up and have not improved. She states the pain is moderate, throbbing, tight in character, and is located in the occipital region bilaterally. The patient denies any visual and audio disturbances, nausea, and vomiting. She recalls 2 similar headaches in the past month. She has no other relevant medical history. Current medications are alendronate and a daily multivitamin. The patient works long hours as a corporate attorney. A review of systems is significant for mild photophobia. Her temperature is 37.0°C (98.6°F), the blood pressure is 110/70 mm Hg, the pulse is 70/min, the respiratory rate is 18/min, and the oxygen saturation is 98% on room air. On physical exam, the patient is alert and oriented. There is moderate tenderness to palpation diffusely over the upper posterior cervical muscles and occipital region of the scalp. The remainder of the physical exam is normal. Laboratory tests are normal. Urine pregnancy test is negative. What is the next best step in management?
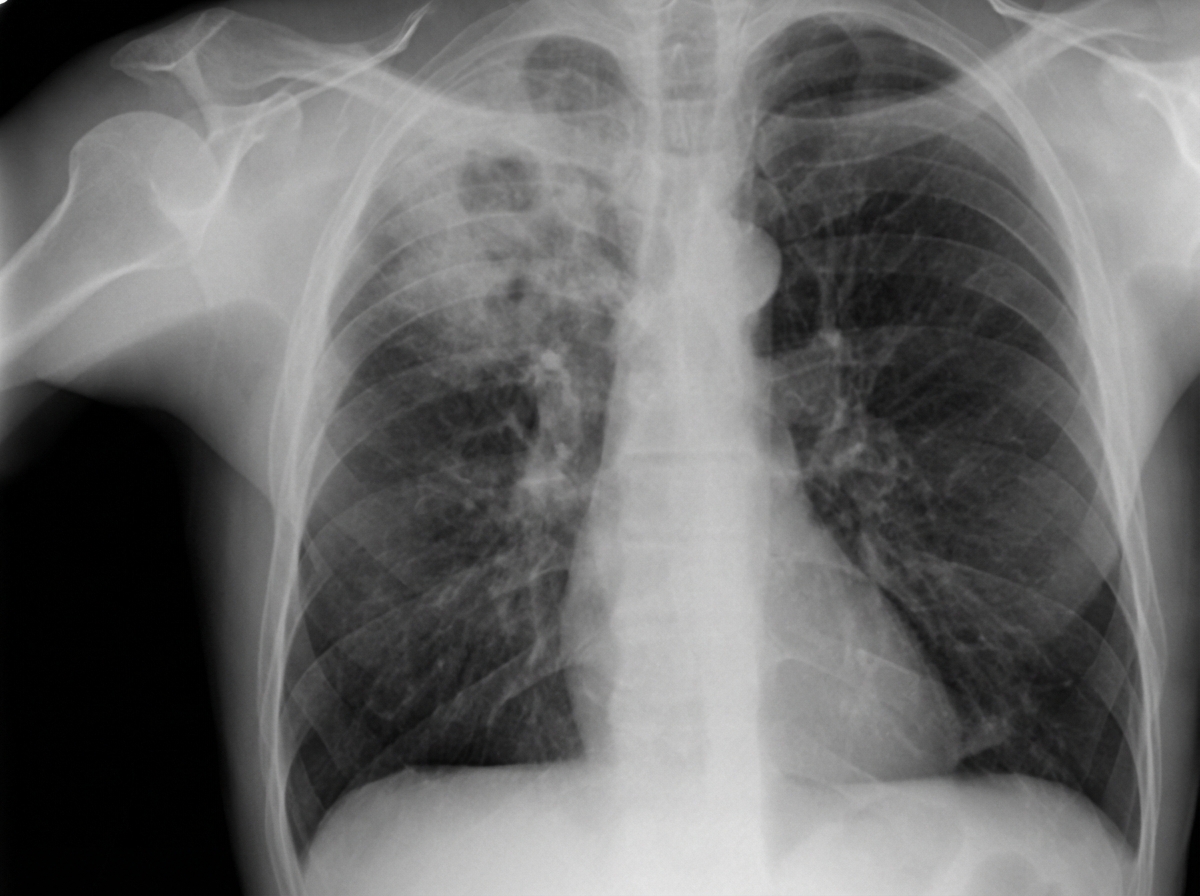
A 38-year-old man comes to the physician because of a 1-month history of fever and a cough productive of a moderate amount of yellowish sputum. He has had a 6-kg (13-lb) weight loss during this period. He emigrated from the Middle East around 2 years ago. His father died of lung cancer at the age of 54 years. He has smoked one pack of cigarettes daily for 18 years. He appears malnourished. His temperature is 38.1°C (100.6°F), pulse is 101/min, and blood pressure is 118/72 mm Hg. Crackles are heard on auscultation of the chest. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. Laboratory studies show: Hemoglobin 12.3 g/dL Leukocyte count 13,200/mm3 Platelet count 330,000/mm3 Erythrocyte sedimentation rate 66 mm/h Serum Urea nitrogen 16 mg/dL Glucose 122 mg/dL Creatinine 0.9 mg/dL Urinalysis is within normal limits. An x-ray of the chest is shown. Which of the following is the most appropriate next step in management?
A 32-year-old woman comes to the physician because of weight gain, generalized weakness, and irregular menstrual cycles for the past 16 months. She began having symptoms of insomnia and depression 10 months ago. More recently, she has been having difficulties rising from a chair. She has a 2-year history of hypertension. Current medications include citalopram and hydrochlorothiazide. She is 168 cm (5 ft 6 in) tall and weighs 100 kg (220 lb). BMI is 36 kg/m2. Her pulse is 92/min, respirations are 18/min, and blood pressure is 134/76 mm Hg. She appears tired and has a full, plethoric face and central obesity. Examination of the skin shows violaceous linear striations on her lower abdomen. Two midnight serum cortisol studies show measurements of 288 μg/L and 253 μg/L (N < 90); a 24-hour urinary cortisol measurement was 395 μg (N < 300). Upon follow-up laboratory examination, the patient's serum ACTH levels were also elevated at 136 pg/mL (N = 7–50). Which of the following is the most appropriate next step in evaluation?
A 17-year-old male presents to your office complaining of polyuria, polydipsia, and unintentional weight loss of 12 pounds over the past 3 months. On physical examination, the patient is tachypneic with labored breathing. Which of the following electrolyte abnormalities would you most likely observe in this patient?
A 53-year-old Asian woman comes to the physician because of a 2-month history of severe pain in her right leg while walking. She used to be able to walk a half-mile (800-m) to the grocery store but has been unable to walk 200 meters without stopping because of the pain over the past month. She can continue to walk after a break of around 5 minutes. She has hypertension, atrial fibrillation, and type 2 diabetes mellitus. She has smoked one pack of cigarettes daily for the past 32 years. Current medications include metformin, enalapril, aspirin, and warfarin. Vital signs are within normal limits. Examination shows an irregularly irregular pulse. The right lower extremity is cooler than the left lower extremity. The skin over the right leg appears shiny and dry. Femoral pulses are palpated bilaterally; pedal pulses are diminished on the right side. Which of the following is the most appropriate next step in management?
A 68-year-old woman comes to the physician for a follow-up visit for elevated blood pressure. Two weeks ago, her blood pressure was 154/78 mm Hg at a routine visit. Subsequent home blood pressure measurements at days 5, 10, and 14 have been: 156/76 mm Hg, 158/80 mm Hg, and 160/80 mm Hg. She has trouble falling asleep but otherwise feels well. She had a cold that resolved with over-the-counter medication 2 weeks ago. She has a history of primary hypothyroidism and a cyst in the right kidney, which was found incidentally 20 years ago. She takes levothyroxine. She is 178 cm (5 ft 10 in) tall and weighs 67 kg (148 lb); BMI is 21.3 kg/m2. Her pulse is 82/min, and blood pressure is 162/79 mm Hg. Examination shows no abnormalities. Laboratory studies, including thyroid function studies, serum electrolytes, and serum creatinine, are within normal limits. Which of the following is the most likely underlying cause of this patient's blood pressure findings?
A 58-year-old woman presents to the physician with a throbbing headache. She says she had it for the last year and it’s usually located in the right temporal area. There is localized tenderness over the scalp. During the last 2 weeks, she experienced 3 episodes of transient loss of vision on the right side, without ocular pain. On physical examination, her vital signs are normal. Palpation reveals that the pulsations of the superficial temporal artery on the right side are reduced in amplitude. Laboratory studies show: Blood hemoglobin 10.7 g/dL (6.64 mmol/L) Leukocyte count 8,000/mm3 (8.0 x 109/L) Platelet count 470,000/mm3 (470 x 109/L) Erythrocyte sedimentation rate 60 mm/h (60 mm/h) Which of the following conditions is most likely to co-exist with the presenting complaint in this woman?
A 15-year-old boy is brought to the physician by his father because he has been waking up frequently during the night to urinate. Apart from occasional headaches, he has no other complaints. His family recently emigrated from Tanzania and his medical history is unknown. His father was diagnosed with sickle cell disease at the age of 5. Physical examination shows no abnormalities. Laboratory studies show: Hemoglobin 14.5 g/dL Hematocrit 44% MCV 90 fL Reticulocytes 1.5% A hemoglobin electrophoresis shows: HbA 55% HbS 43% HbF 1% This patient is at greatest risk for which of the following conditions?
A 59-year-old woman comes to the physician because of a 1-month history of episodic cough and shortness of breath. The cough is nonproductive and worsens when she climbs stairs and during the night. She has not had chest pain or palpitations. Eight weeks ago, she had fever, sore throat, and nasal congestion. She has a 10-year history of hypertension. She has smoked half a pack of cigarettes daily for 16 years. Her only medication is enalapril. Her pulse is 78/min, respirations are 18/min, and blood pressure is 145/95 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. Diffuse end-expiratory wheezes are heard on pulmonary auscultation. An x-ray of the chest shows no abnormalities. Spirometry shows an FEV1:FVC ratio of 65% and an FEV1 of 60%. Which of the following is the most likely diagnosis?
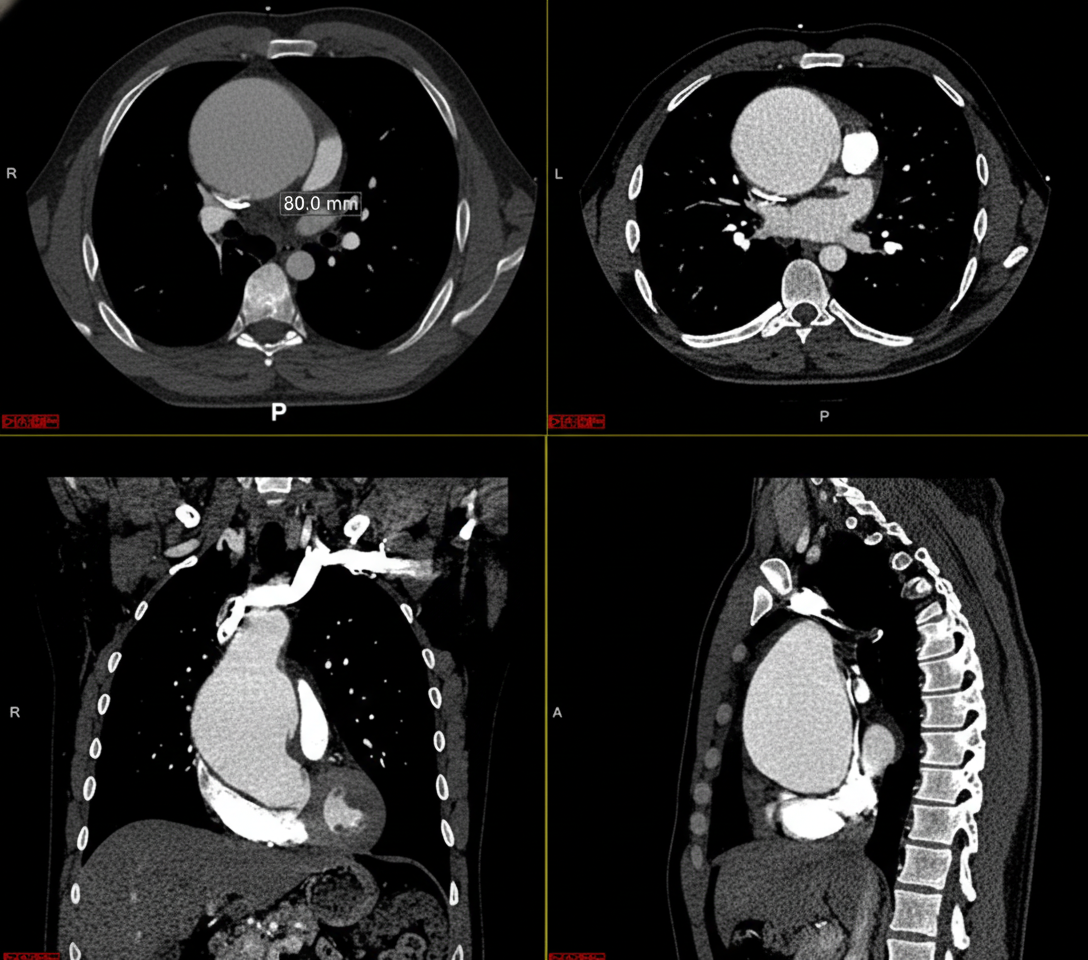
A previously healthy 32-year-old man comes to the physician because of a 1-week history of upper back pain and a sensation of pressure in his chest. He has had no shortness of breath, palpitations, fevers, or chills. He emigrated from Ecuador when he was 5 years old. He does not smoke or drink alcohol. He takes no medications. He is 194 cm (6 ft 4 in) tall and weighs 70.3 kg (155 lb); BMI is 19 kg/m2. His temperature is 37.2°C (99.0°F), pulse is 73/min, respirations are 15/min, and blood pressure is 152/86 mm Hg in the right arm and 130/72 mm Hg in the left arm. Physical examination shows long fingers and toes (arachnodactyly) and a pectus excavatum deformity. Pulmonary examination shows faint inspiratory wheezing bilaterally. A CT scan of the chest with contrast is shown. Which of the following is the most likely underlying cause of this patient's condition?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app