
Cardiology — MCQs

On this page
A 68-year-old female presents to the emergency room with acute onset of dyspnea and hemoptysis. Her past medical history is unremarkable and she has had no prior surgeries. A ventilation-perfusion scan demonstrates a large perfusion defect that is not matched by a ventilation defect in the left lower lobe. Which of the following would you also expect to find in this patient:
A 45-year-old African American woman presents to her family physician for a routine examination. Past medical history is positive for amyloidosis and non-rhythm-based cardiac abnormalities secondary to the amyloidosis. Which of the following cardiac parameters would be expected in this patient?
A 34-year-old man comes to the physician for a routine health maintenance examination. He was diagnosed with HIV 8 years ago. He is currently receiving triple antiretroviral therapy. He is sexually active and uses condoms consistently. He is planning a trip to Thailand with his partner to celebrate his 35th birthday in 6 weeks. His last tetanus and diphtheria booster was given 4 years ago. He received three vaccinations against hepatitis B 5 years ago. He had chickenpox as a child. Other immunization records are unknown. Vital signs are within normal limits. Cardiopulmonary examination shows no abnormalities. Leukocyte count shows 8,700/mm3, and CD4+ T-lymphocyte count is 480 cells/mm3 (Normal ≥ 500); anti-HBs is 150 mIU/mL. Which of the following recommendations is most appropriate at this time?
Two days after admission to the hospital, a 74-year-old man develops confusion and headache. He has also been vomiting over the past hour. His temperature is 36.7°C (98°F), pulse is 98/min, respirations are 22/min, and blood pressure is 140/80 mm Hg. He is lethargic and oriented only to person. Examination shows flushed skin. Fundoscopic examination shows bright red retinal veins. Serum studies show: Na+ 138 mEq/L K+ 3.5 mEq/L Cl- 100 mEq/L HCO3- 17 mEq/L Creatinine 1.2 mg/dL Urea nitrogen 19 mg/dL Lactate 8.0 mEq/L (N = 0.5 - 2.2 mEq/L) Glucose 75 mg/dL Arterial blood gas analysis on room air shows a pH of 7.13. This patient's current presentation is most likely due to complications from treatment of which of the following conditions?
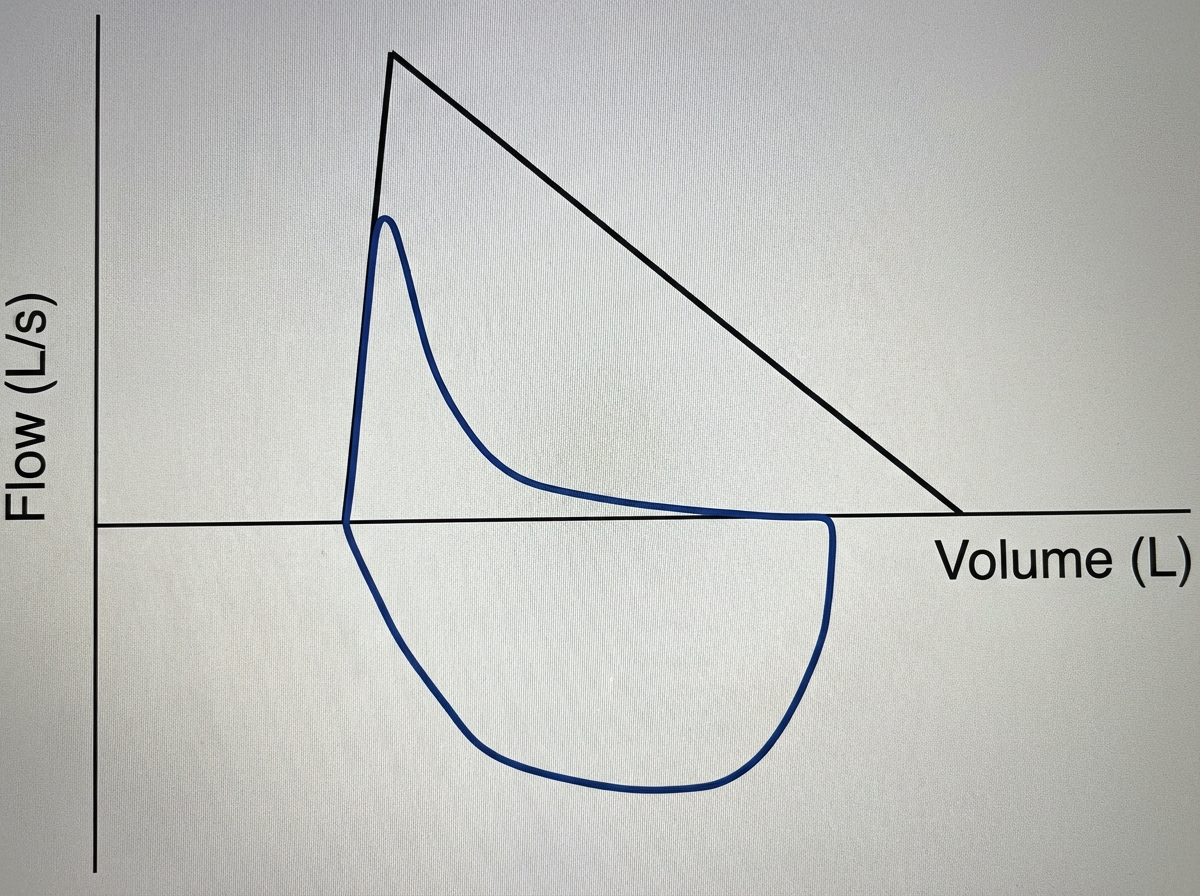
A 63-year-old woman comes to the physician because of worsening shortness of breath, cough, and a 4-kg (8.8-lb) weight loss over the last year. She has no history of serious illness and takes no medications. She has smoked one pack of cigarettes daily for 35 years. Her temperature is 37°C (98.6°F), pulse is 92/min, respirations are 20/min, blood pressure is 124/78 mm Hg, and pulse oximetry on room air shows an oxygen saturation of 93%. Physical examination shows decreased breath sounds. A flow-volume loop obtained via pulmonary function testing is shown. Which of the following is the most likely cause of this patient's respiratory symptoms?
A 30-year-old African American woman comes to the physician because of a 3-month history of increasing shortness of breath, cough, and intermittent fever. She works in a local factory that manufactures components for airplanes. She drinks 2–3 glasses of wine daily and has smoked half a pack of cigarettes daily for the past 5 years. Physical examination shows a purple rash on her cheeks and nose. An x-ray of the chest shows bilateral hilar adenopathy and a calcified nodule in the left lower lobe. A bronchoalveolar lavage shows a CD4:CD8 T-lymphocyte ratio of 10:1 (N=2:1). A biopsy of the nodule shows a noncaseating granuloma. Which of the following is the strongest predisposing factor for the development of this patient's condition?
A 25-year-old man is in the middle of an ascent up a mountain, at an elevation of about 4,500 meters. This is the 4th day of his expedition. His friend notices that in the last few hours, he has been coughing frequently and appears to be short of breath. He has used his albuterol inhaler twice in the past 4 hours, but it does not seem to help. Within the past hour, he has coughed up some frothy, slightly pink sputum and is now complaining of nausea and headache. Other than his asthma, which has been well-controlled on a steroid inhaler, he is healthy. Which of the following is the most likely cause of this man’s symptoms?
A 45-year-old woman presents to the office with a complaint of generalized weakness that has been getting worse over the last few months. She says that she just does not have the energy for her daily activities. She gets winded quite easily when she takes her dog for a walk in the evening. She says that her mood is generally ok and she gets together with her friends every weekend. She works as a teacher at a local elementary school and used to have frequent headaches while at work. Her husband is a commercial pilot and is frequently away for extended periods of time. Her only son is a sophomore in college and visits her every other week. She has had issues in the past with hypertension, but her blood pressure is currently well-controlled because she is compliant with her medication. She is currently taking atorvastatin and lisinopril. The blood pressure is 130/80 mm Hg, the pulse is 90/min, the temperature is 36.7°C (98.0°F), and the respirations are 16/min. On examination, she appears slightly pale and lethargic. Her ECG today is normal and recent lab work shows the following: Serum creatinine 1.5 mg/dL Estimated GFR 37.6 mL/min Hemoglobin (Hb%) 9 mg/dL Mean corpuscular hemoglobin (MCH) 27 pg Mean corpuscular hemoglobin concentration (MCHC) 36 g/dL Mean corpuscular volume (MCV) 85 fL Reticulocyte count 0.1% Erythrocyte count 2.5 million/mm3 Serum iron 160 μg/dL Serum ferritin 150 ng/mL Total iron binding capacity 105 μg/dL Serum vitamin B12 254 pg/mL Serum folic acid 18 ng/mL Thyroid stimulating hormone 3.5 μU/mL Which of the following will most likely help her?
A 54-year-old man presents to his primary care physician for back pain. His back pain worsens with standing for a prolonged period of time or climbing down the stairs and improves with sitting. Medical history is significant for hypertension, type II diabetes mellitus, and hypercholesterolemia. Neurologic exam demonstrates normal tone, 5/5 strength, and a normal sensory exam throughout the bilateral lower extremity. Skin exam is unremarkable and dorsalis pedis and posterior tibialis pulses are 3+. Which of the following is the best next step in management?
A 36-year-old man presents to the physician with difficulty in breathing for 3 hours. There is no history of chest pain, cough or palpitation. He is a chronic smoker and underwent elective cholecystectomy one month back. There is no history of chronic or recurrent cough, wheezing or breathlessness. His temperature is 38.2°C (100.8°F), pulse is 108/min, blood pressure is 124/80 mm Hg, and respirations are 25/min. His arterial oxygen saturation is 98% in room air as shown by pulse oximetry. After a detailed physical examination, the physician orders a plasma D-dimer level, which was elevated. A contrast-enhanced computed tomography (CT) of the chest shows a filling defect in a segmental pulmonary artery on the left side. Which of the following signs is most likely to have been observed by the physician during the physical examination of this patient’s chest?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app