
Cardiology — MCQs

On this page
A 56-year-old man comes to the clinic complaining of back pain for the past 1 month. The pain is described as a dull ache that intensifies intermittently to an 8/10 in severity about 1-2 times a day. It intensified about 2 weeks ago following a fall during a ski trip. He reports that he noticed some pain at his buttocks and lower back following the fall but he wasn’t bothered by it. Hot packs and Tylenol seem to alleviate the pain somewhat. He denies lower extremity weakness, loss of sensation, fever, incontinence, or prior cancers; however, he reveals that his cousin was recently diagnosed with prostate cancer. Physical examination demonstrates normal range of motion and diffuse tenderness at the L4/L5 region with no point tenderness or vertebral step-offs. What is the next best step in the management of this patient?
A 32-year-old man comes to the emergency department because of sharp chest pain for 3 days. The pain is retrosternal, 8 out of 10 in intensity, increases with respiration, and decreases while sitting upright and leaning forward. He has nausea and myalgia. He has not had fever or a cough. He has asthma and was treated for bronchitis 6 months ago with azithromycin. His mother has hypertension. He uses an over-the-counter inhaler. His temperature is 37.3°C (99.1°F), pulse is 110/min, and blood pressure is 130/84 mm Hg. Breath sounds are normal. Cardiac examination shows a high-pitched grating sound between S1 and S2. The remainder of the examination shows no abnormalities. Serum studies show: Urea nitrogen 16 mg/dl Glucose 103 mg/dL Creatinine 0.7 mg/dL Troponin I 0.230 ng/mL (N < 0.1 ng/mL) An ECG shows diffuse ST elevations in all leads. The patient is at increased risk for which of the following conditions?
A 70-year-old man presents to the clinic with right-sided chest pain and difficulty breathing for the past 10 days. When it began, the pain was mild, but as time went on, it increased to a level at which the man found it difficult to breathe. Two years ago, he was diagnosed with clear cell carcinoma of the kidney. Vital signs include: pulse rate is 72/min, blood pressure is 122/80 mm Hg, respiratory rate is 16/min, and temperature is 37.0°C (98.6°F). On physical examination, the trachea appears to have deviated to the left, respiratory movements are diminished, there is decreased resonance on percussion, and there is an absence of breath sounds over the right hemithorax. Which of the following is the most likely clinical diagnosis in this patient?
A 66-year-old white man comes to the physician because of a 10-day history of fatigue and lower leg swelling. Over the past 6 months, he has had a 3.6-kg (8-lb) weight loss. He has chronic bronchitis and uses an albuterol inhaler as needed. He has smoked one pack of cigarettes daily for 44 years and drinks one alcoholic beverage daily. His temperature is 37°C (98.6°F), pulse is 88/min, and blood pressure is 120/75 mm Hg. He appears thin. Examination shows 2+ pretibial edema bilaterally. Cardiopulmonary examination shows no abnormalities. Laboratory studies show: Hemoglobin 11.2 g/dL Leukocyte count 8500/mm3 Platelet count 130,000/mm3 Serum Urea nitrogen 23 mg/dL Glucose 77 mg/dL Creatinine 1.6 mg/dL Albumin 1.8 mg/dL Total cholesterol 475 mg/dL Urine Blood negative Glucose negative Protein 4+ WBC 0–1/hpf Fatty casts numerous An x-ray of the chest shows a right upper lobe density. A CT scan of the chest shows a 2.5 x 3.5 x 2-cm right upper lobe mass. Which of the following is the most likely diagnosis?
A 17-year-old African-American male presents to his family physician after noticing red-tinged urine the week before, when he was suffering from a cold. The patient states that he had experienced that before. His father is with him and says that this happens to him on occasion as well. What is the most likely diagnosis for this patient?
An 80-year-old male with known metastatic prostate cancer presents to your office with vague complaints of "achy bones." Strangely, he refers to you using the name of another physician. On physical exam, he is afebrile, but mildly tachycardic at 100 beats/min. Mucous membranes are dry. Cardiac exam shows regular rhythm and no murmurs. The patient has diffuse, nonfocal abdominal pain. He cannot articulate the correct date. You check the patient's serum calcium level, which is found to be 15.3 mg/dL. What is the best next step in management?
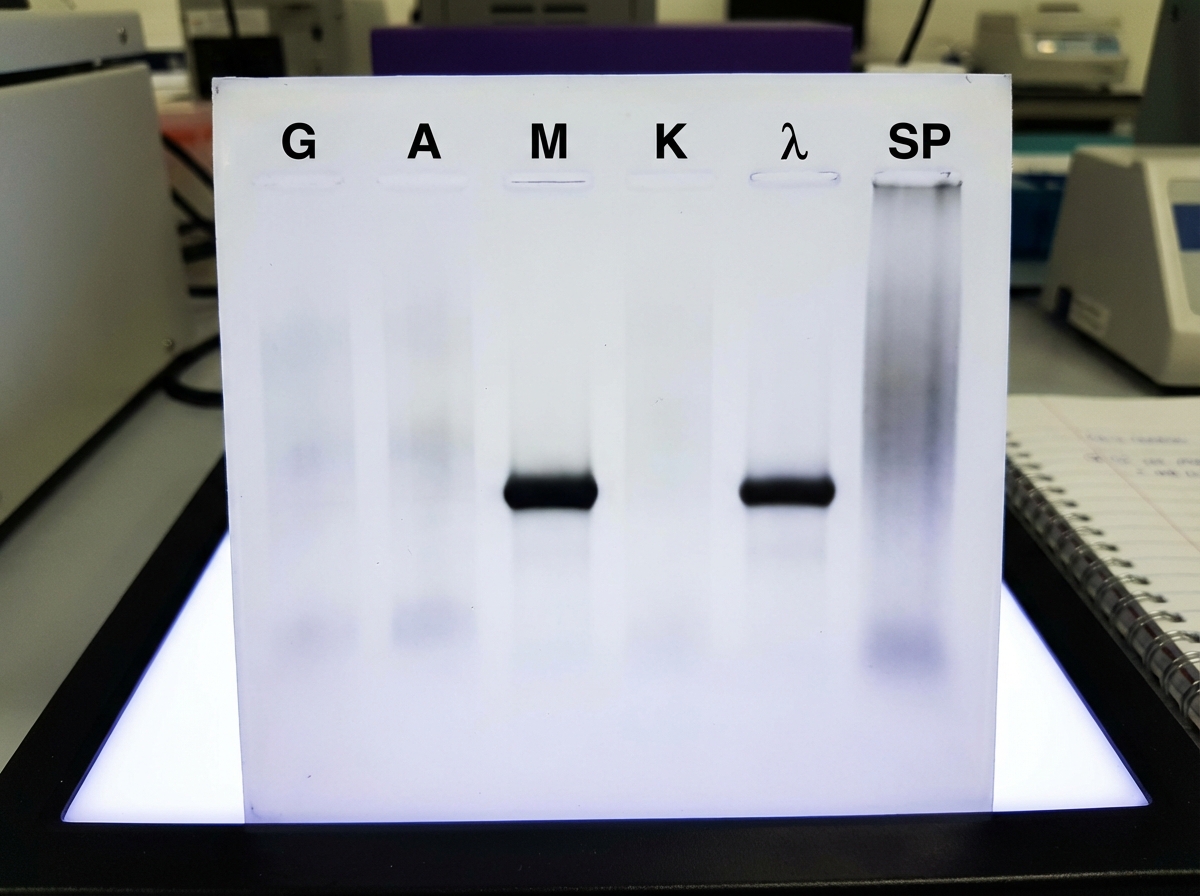
A 78-year-old man presents to the emergency department because of confusion that started 2 hours ago. The patient’s daughter says that he has had blurred vision for several days. His right leg became weak 10 days ago, and he couldn’t walk for a few days before recovering. He was diagnosed with monoclonal gammopathy of undetermined significance 2 years ago. His temperature is 36.2°C (97.2°F), pulse is 75/min, respirations are 13/min, and blood pressure is 125/70 mm Hg. He also has gingival bleeding. Cervical lymphadenopathy is palpated on physical exam. Both the liver and spleen are palpated 5 cm below the costal margins. The serum protein electrophoresis with immunofixation is shown. Urine electrophoresis shows no abnormalities. A skeletal survey shows no abnormalities. Which of the following best explains these findings?
A 47-year-old woman comes to the physician because of a 1-month history of progressive weakness. She has had increased difficulty climbing stairs and standing from a seated position. She takes no medications. Neurologic examination shows weakness of the proximal muscles. Skin examination shows diffuse erythema of the upper back, posterior neck, and shoulders. A photograph of the patient's eye is shown. Antibodies against which of the following are most likely to be present in this patient?

A 12-year-old boy is brought by his mother to the emergency room because of a swollen, hot, and tender knee that he sustained after falling on his way home. He has never had a swollen joint before; however, he has had frequent nosebleeds throughout his life. His mother is worried because they live with her parents who are currently on blood thinners. Every morning she puts the blood thinner pill in the boy's grandfather's milk and was concerned that she may have switched it this morning. Family history reveals a number of uncles who have had bleeding disorders; however, the mother does not know the exact disorder suffered by these relatives. A hematologic panel reveals the following findings: Bleeding time: Increased Prothrombin time: 12 seconds Partial thromboplastin time (PTT): 55 seconds PTT after factor mixing study: 37 seconds Which of the following most likely explains the abnormal partial thromboplastin time in this patient?
A 42-year-old man comes to the physician for a health maintenance examination. He has had generalized fatigue and muscle aches since his previous visit 6 months ago. He has hypertension and gastroesophageal reflux disease. Current medications include amlodipine and omeprazole. His temperature is 37.1°C (98.1°F), pulse is 88/min and blood pressure is 156/102 mm Hg. Physical examination shows no abnormalities. Serum studies show: Na+ 143 mEq/L K+ 2.3 mEq/L Cl- 100 mEq/L HCO3- 31 mEq/L Urea nitrogen 14 mg/dL Creatinine 1 mg/dL His blood pressure medication is discontinued. One week later his plasma aldosterone concentration is 35 ng/dL (N=3.6 - 24.0 ng/dL) and plasma renin activity is 0.4 ng/mL/h (N=0.3 to 4.2 ng/mL/h). An oral sodium loading test over 3 days fails to reduce aldosterone. A contrast-enhanced CT scan of the abdomen and pelvis shows a 3-cm, homogenous, right-sided adrenal mass with rapid contrast washout. He is counseled about his treatment options and chooses to pursue surgery. Which of the following is the most appropriate next step in management?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app