
Cardiology — MCQs

On this page
A 48-year-old woman presents to her primary care physician with complaints of persistent fatigue, dizziness, and weight loss for the past 3 months. She has a history of hypothyroidism and takes thyroxine replacement. Her blood pressure is 90/60 mm Hg in a supine position and 65/40 mm Hg while sitting, temperature is 36.8°C (98.2°F), and pulse is 75/min. On physical examination, there is a mild increase in thyroid size, with a rubbery consistency. Her skin shows diffuse hyperpigmentation, more pronounced in the oral mucosa and palmar creases. Which of the following best represent the etiology of this patient’s condition?
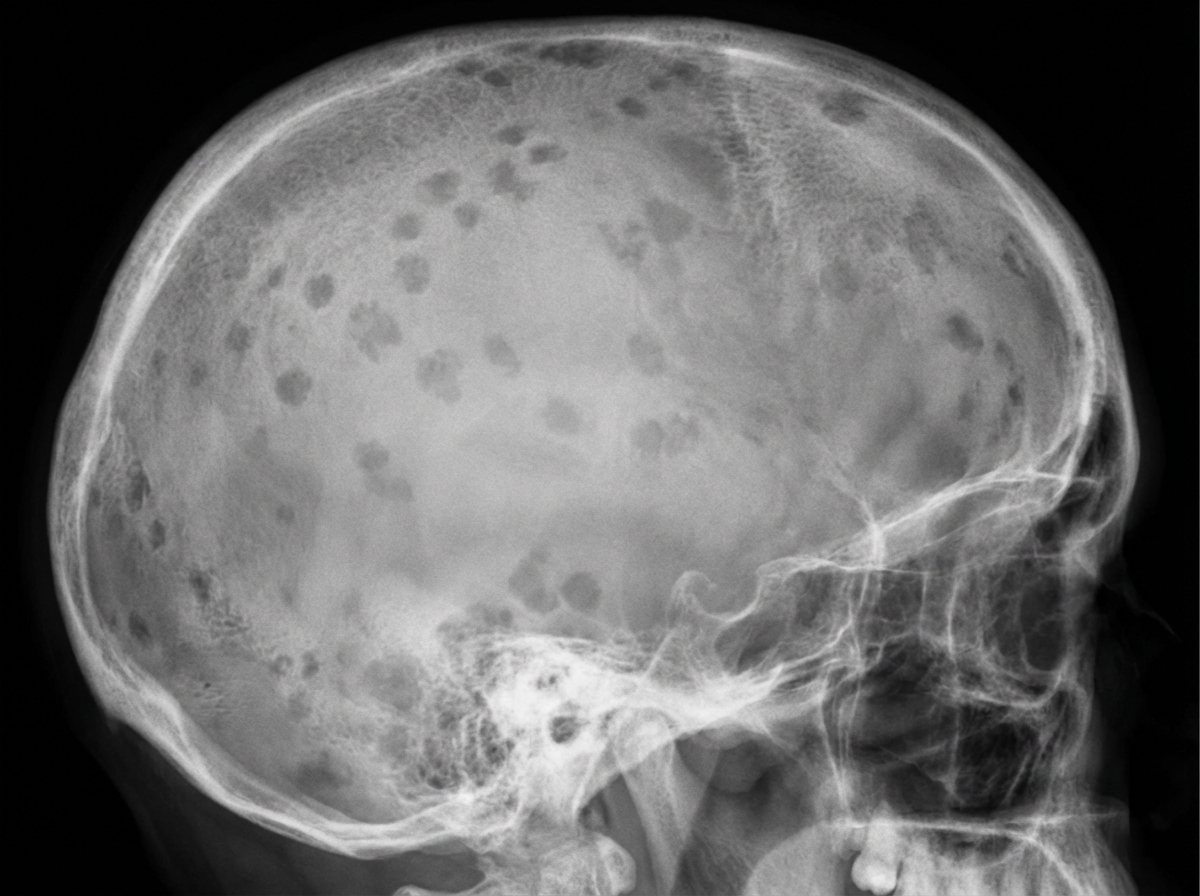
A 71-year-old African American man is brought to the emergency department with a worsening productive cough and dyspnea for 2 days. He has had generalized bone pain for 2 months. He was admitted for pyelonephritis last month. He also received outpatient treatment for pneumonia almost 2 months ago. Over the past 2 months, he has been taking over-the-counter ibuprofen for pain as needed. He appears anxious. The vital signs include: temperature 38.8°C (101.8°F), pulse 95/min, respiratory rate 20/min, and blood pressure 155/90 mm Hg. The conjunctivae are pale. Crackles are heard in the right lower lobe. The cardiac examination shows no abnormalities. The laboratory studies show the following: Hemoglobin 9 g/dL Mean corpuscular volume 95 μm3 Leukocyte count 13,500/mm3 Segmented neutrophils 75% Lymphocytes 25% Platelet count 240,000/mm3 ESR 85 mm/hr Serum Na+ 135 mEq/L K+ 4.2 mEq/L Cl− 113 mEq/L HCO3− 20 mEq/L Ca+ 12.4 mg/dL Albumin 4 g/dL Urea nitrogen 38 mg/dL Creatinine 2.2 mg/dL A chest X-ray shows a right lower lobe opacity and blurring of the ipsilateral diaphragmatic dome. Skull and pelvic X-rays are performed (see image). Which of the following is the most likely underlying cause of this patient’s recent infections?
A 23-year-old woman presents with ongoing diplopia for 1 week. She has noticed that her diplopia is more prominent when she looks at objects in her periphery. It does not present when looking straight ahead. She does not have a fever, headache, ocular pain, lacrimation, blurring of vision, or changes in her color vision. She is a college student and is otherwise healthy. The neurological examination reveals that when she looks to the left, her right eye does not adduct while her left eye abducts with nystagmus. Furthermore, when she looks to the right, her left eye does not adduct while her right eye abducts with prominent nystagmus. Her pupils are bilateral, equal and reactive to light and accommodation. The convergence is normal. The rest of the cranial nerve examination is unremarkable. What is the next best step in the management of this patient?
A 65-year-old man with hypertension and type 2 diabetes mellitus is brought to the emergency department 20 minutes after the onset of severe anterior chest pain and shortness of breath. He has smoked one pack of cigarettes daily for 30 years. He appears distressed. His pulse is 116/min, respirations are 22/min, and blood pressure is 156/88 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. A grade 3/6, high-pitched, blowing, diastolic murmur is heard over the right upper sternal border. Which of the following is the most likely cause of this patient's symptoms?
A 39-year-old woman presents with progressive weakness, exercise intolerance, and occasional dizziness for the past 3 months. Past medical history is unremarkable. She reports an 18-pack-year smoking history and drinks alcohol rarely. Her vital signs include: temperature 36.6°C (97.8°F), blood pressure 139/82 mm Hg, pulse 98/min. Physical examination is unremarkable. Her laboratory results are significant for the following: Hemoglobin 9.2 g/dL Erythrocyte count 2.1 million/mm3 Mean corpuscular volume (MCV) 88 μm3 Mean corpuscular hemoglobin (MCH) 32 pg/cell Leukocyte count 7,500/mm3 Which of the following is the best next step in the management of this patient’s condition?
A 45-year-old woman comes to the physician because of fatigue, irregular menses, and recurrent respiratory infections for the past 6 months. Her blood pressure is 151/82 mm Hg. Physical examination shows a round face, thinning of the skin, and multiple bruises on her arms. Further studies confirm the diagnosis of an ACTH-secreting pituitary adenoma. This patient is at greatest risk for which of the following?
A 54-year-old man comes to the emergency department because of a 3-week history of intermittent swelling of his left arm and feeling of fullness in his head that is exacerbated by lying down and bending over to tie his shoes. Physical examination shows left-sided facial edema and distention of superficial veins in the neck and left chest wall. Which of the following is the most likely cause of this patient's symptoms?
A 45-year-old male presents to his primary care physician for complaints of dizziness. The patient reports he experiences room-spinning dizziness lasting several hours at a time, approximately 2-3 times a month, starting 3 months ago. Upon questioning, the patient also reports right sided diminished hearing, tinnitus, and a sensation of ear fullness. His temperature is 99 deg F (37.2 deg C), pulse 70/min, respirations 12, blood pressure 130 mmHg/85 mmHg, SpO2 99%. You decide to order an audiometric evaluation. What is the most likely finding of the audiogram?
A 32-year-old man comes to the physician for a follow-up examination 1 week after being admitted to the hospital for oral candidiasis and esophagitis. His CD4+ T lymphocyte count is 180 cells/μL. An HIV antibody test is positive. Genotypic resistance assay shows the virus to be susceptible to all antiretroviral therapy regimens and therapy with dolutegravir, tenofovir, and emtricitabine is initiated. Which of the following sets of laboratory findings would be most likely on follow-up evaluation 3 months later? $$$ CD4 +/CD8 ratio %%% HIV RNA %%% HIV antibody test $$$
A 62-year-old woman comes to the physician because of involuntary, rhythmic movements of her hands for the past 5 months. Her symptoms initially affected her left hand only, but now both hands are affected. She also reports that her symptoms are worse at rest and that performing tasks such as tying her shoelaces and writing have become more difficult. Her husband thinks that she has been more withdrawn lately. She used to drink a half a bottle of sherry every day for the past 18 years but has not consumed alcohol in the past year. She has chronic liver disease, hypertension, and peripheral artery disease. Current medications include aspirin and propanolol. She appears anxious. She is oriented to time, place, and person. Her temperature is 37°C (98.6°F), pulse is 98/min, and blood pressure is 144/82 mm Hg. Examination shows a rhythmic, low-frequency tremor that is more prominent in the left hand. Range of motion in the arms and legs is normal. Increased resistance to passive flexion and extension is present in the left upper limb. Muscle strength is 4/5 in all limbs. Sensations to pinprick and light touch are preserved. The finger-to-nose test is normal bilaterally. Which of the following is the most likely underlying cause of this patient's symptoms?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app