
Cardiology — MCQs

On this page
A 14-year-old male presents to his primary care physician with complaints of shortness of breath and easy fatigability when exercising for extended periods of time. He also reports that, when he exercises, his lower legs and feet turn a bluish-gray color. He cannot remember visiting a doctor since he was in elementary school. His vital signs are as follows: HR 72, BP 148/65, RR 14, and SpO2 97%. Which of the following murmurs and/or findings would be expected on auscultation of the precordium?
A 52-year-old man comes to the physician for a routine medical check-up. The patient feels well. He has hypertension, type 2 diabetes mellitus, and recurrent panic attacks. He had a myocardial infarction 3 years ago. He underwent a left inguinal hernia repair at the age of 25 years. A colonoscopy 2 years ago was normal. He works as a nurse at a local hospital. He is married and has two children. His father died of prostate cancer at the age of 70 years. He had smoked one pack of cigarettes daily for 25 years but quit following his myocardial infarction. He drinks one to two beers on the weekends. He has never used illicit drugs. Current medications include aspirin, atorvastatin, lisinopril, metoprolol, fluoxetine, metformin, and a multivitamin. He appears well-nourished. Temperature is 36.8°C (98.2°F), pulse is 70/min, and blood pressure is 125/75 mm Hg. Lungs are clear to auscultation. Cardiac examination shows a high-frequency, mid-to-late systolic murmur that is best heard at the apex. The abdomen is soft and nontender. The remainder of the physical examination shows no abnormalities. Which of the following is the most likely diagnosis?
A 68-year-old man presents to his primary care physician for a routine checkup. He currently has no complaints. During routine blood work, he is found to have a slightly elevated calcium (10.4 mg/dL) and some findings of plasma cells in his peripheral blood smear (less than 10%). His physician orders a serum protein electrophoresis which demonstrates a slight increase in gamma protein that is found to be light chain predominate. What is the most likely complication for this patient as this disease progresses if left untreated?
A 67-year-old woman presents to her primary care physician because she has been feeling increasingly fatigued over the last month. She has noticed that she gets winded halfway through her favorite walk in the park even though she was able to complete the entire walk without difficulty for years. She recently moved to an old house and started a new Mediterranean diet. Her past medical history is significant for hypertension and osteoarthritis for which she underwent a right hip replacement 2 years ago. Physical exam reveals conjunctival pallor as well as splenomegaly. Labs are obtained and the results are shown below: Hemoglobin: 9.7 g/dL (normal: 12-15.5 g/dL) Mean corpuscular volume: 91 µm^3 (normal: 80-100 µm^3) Direct Coombs test: positive Indirect Coombs test: positive Peripheral blood smear reveals spherical red blood cells. The disorder that is most likely responsible for this patient's symptoms should be treated in which of the following ways?
A 22-year-old woman comes to the physician for gradual worsening of her vision. Her father died at 40 years of age. She is 181 cm (5 ft 11 in) tall and weighs 69 kg (152 lb); BMI is 21 kg/m2. A standard vision test shows severe myopia. Genetic analysis shows an FBN1 gene mutation on chromosome 15. This patient is at greatest risk of mortality due to which of the following causes?
A 65-year-old male presents to the emergency department with a 2-day onset of right-lower quadrant and right flank pain. He also states that over this period of time he has felt dizzy, light-headed, and short of breath. He denies any recent trauma or potential inciting event. His vital signs are as follows: T 37.1 C, HR 118, BP 74/46, RR 18, SpO2 96%. Physical examination is significant for an irregularly irregular heart rhythm as well as bruising over the right flank. The patient's medical history is significant for atrial fibrillation, hypertension, and hyperlipidemia. His medication list includes atorvastatin, losartan, and coumadin. IV fluids are administered in the emergency department, resulting in an increase in blood pressure to 100/60 and decrease in heart rate to 98. Which of the following would be most useful to confirm this patient's diagnosis and guide future management?
A 27-year-old woman presents to her primary care physician for a wellness checkup. She states that she is currently doing well but is unable to engage in exercise secondary to her asthma. Her asthma is well-controlled at baseline, and her symptoms only arise when she is trying to exercise once a week at volleyball practice. She is currently only using an albuterol inhaler once a month. The patient’s physical exam is notable for good bilateral air movement without wheezing on pulmonary exam. Which of the following is the best next step in management?
A 60-year-old man presents to the clinic for his annual check-up. The patient says that he has occasional leg cramps, and his legs feel heavy especially after standing for long hours to teach his classes. His past medical history is significant for hypertension which is controlled by metoprolol and lisinopril. He has smoked half a pack of cigarettes daily for the past 30 years. He does not drink alcohol. Family history is significant for myocardial infarction (MI) in his father at the age of 55 years. The blood pressure is 130/80 mm Hg and the pulse rate is 78/min. On physical examination, there are tortuosities of the veins over his lower limb, more pronounced over the left leg. Peripheral pulses are 2+ on all extremities and there are no skin changes. Strength is 5 out of 5 in all extremities bilaterally. Sensation is intact. No pain in the dorsiflexion of the foot. The rest of the examination and the laboratory tests are normal. Which of the following best describes the pathophysiology responsible for this patient’s symptoms?
An 18-year-old man is hospitalized after a suicide attempt, his 6th such attempt in the last 4 years. He was diagnosed with depression 5 years ago, for which he takes fluoxetine. He is currently complaining of severe and worsening left knee swelling and pain since he attempted suicide by jumping out of his second-story bedroom window. He sustained minor injuries at the time, primarily lacerations to his arms and knees, and he was admitted to the hospital’s psychiatric unit. His blood pressure is 110/72 mm Hg, heart rate is 88/min, and temperature is 38°C (100.4°F). On examination, the knee is erythematous and edematous, and it feels warm to the touch. The patient’s lab studies reveal a hemoglobin level of 11.9 g/dL, leukocyte count of 11,200/µL, and a platelet count of 301,000/µL. Arthrocentesis yields 15 mL of fluid with a leukocyte count of 61,000/µL, 93% neutrophils, and an absence of crystals under polarized light microscopy. A gram stain of joint fluid is negative; however, mucosal, blood and synovial fluid cultures are still pending. Which of the following is the most appropriate next step in the management of this patient?
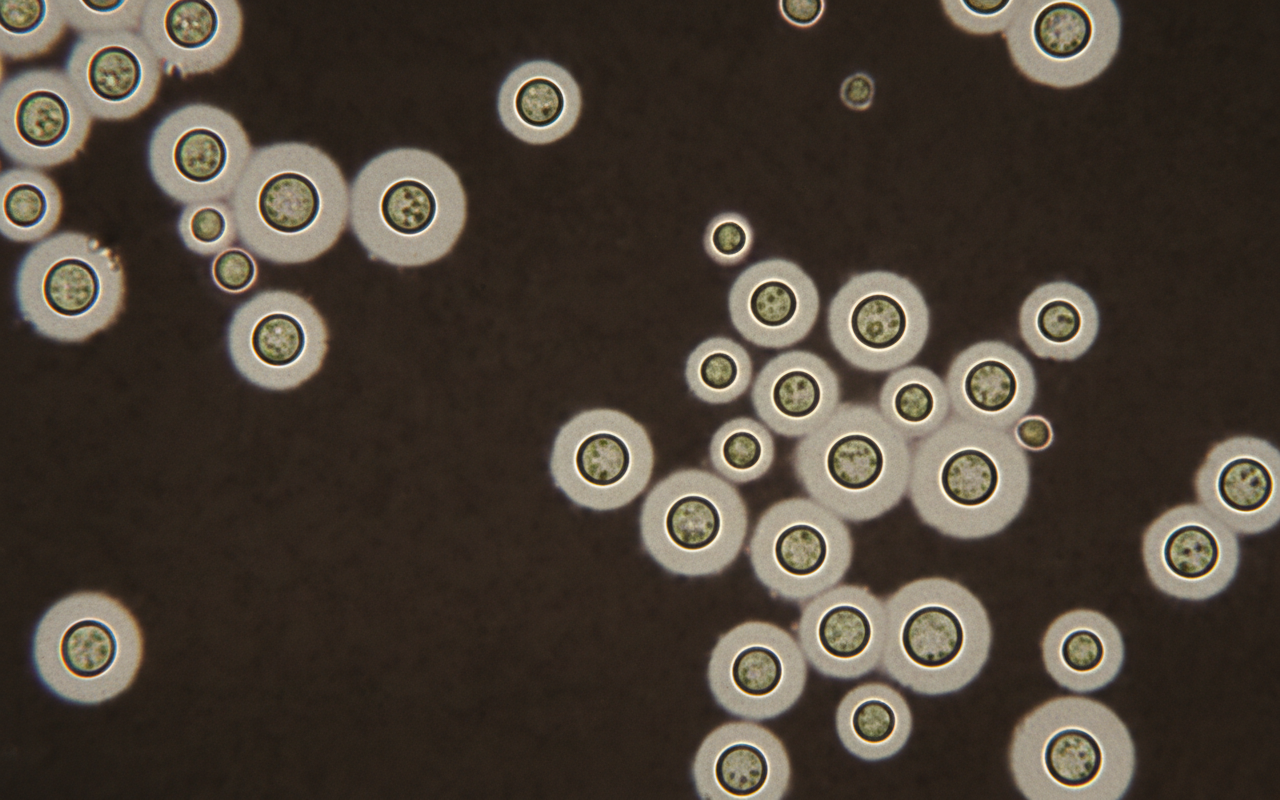
A 40-year-old woman with HIV infection presents to the emergency department because of a 4-week history of progressively worsening fatigue and headache. On mental status examination, the patient is somnolent and oriented only to person. Her CD4+ lymphocyte count is 80/mm3 (N = 500). Analysis of this patient's cerebrospinal fluid (CSF) shows a leukocyte count of 30/mm3 (60% lymphocytes), a protein concentration of 52 mg/dL, and a glucose concentration of 37 mg/dL. An India ink stain of the CSF is shown. Which of the following characteristics would also point towards the most likely cause?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app