
Cardiology — MCQs

On this page
A 75-year-old woman with late-onset autoimmune diabetes mellitus, rheumatoid arthritis, coronary artery disease, and idiopathic pulmonary fibrosis presents to the ship medic with altered mental status. While on her current cruise to the Caribbean islands, she experienced nausea, vomiting, and diarrhea. She takes aspirin, simvastatin, low-dose prednisone, glargine, and aspart. She is allergic to amoxicillin and shellfish. She works as a greeter at a warehouse and smokes 5 packs/day. Her temperature is 100.5°F (38.1°C), blood pressure is 90/55 mmHg, pulse is 130/min, and respirations are 30/min. Her pupils are equal and reactive to light bilaterally. Her lungs are clear to auscultation bilaterally, but her breath has a fruity odor. She has an early systolic murmur best appreciated at the left upper sternal border. She has reproducible peri-umbilical tenderness. Which of the following will most likely be present in this patient?
A 69-year-old man presents with granulomatosis with polyangiitis diagnosed about 8 months ago. He has been on high-dose prednisone (60 mg/day) since diagnosis and states that his symptoms are well controlled. He is presenting today for a general follow up visit. His temperature is 99.0°F (37.2°C), blood pressure is 184/104 mmHg, pulse is 88/min, respirations are 12/min, and oxygen saturation is 98% on room air. His physical examination is notable for the finding in Figure A, and recent labs show a serum potassium of 3.1 mEq/L and a urine potassium-to-creatinine ratio consistent with renal potassium wasting, indicating significant mineralocorticoid activity from his high-dose corticosteroid therapy. Which of the following would be found in this patient on serum laboratory studies?

A 15-year-old boy is brought to the office by his mother with complaints of facial puffiness and smoky urine. The mother noticed puffiness on her son’s face a week ago, and it has been progressively worsening since then. She also states that her son had a sore throat 3 weeks ago. The patient does not have fever/chills, changes in urinary frequency, or abdominal discomfort. On physical examination, facial edema is noted. The vital signs include: blood pressure 145/85 mm Hg, pulse 96/min, temperature 36.7°C (98.1°F), and respiratory rate 20/min. A complete blood count report shows: Hemoglobin 10.1 g/dL RBC 4.9 million cells/µL Hematocrit 46% Total leukocyte count 6,800 cells/µL Neutrophils 70% Lymphocytes 26% Monocytes 3% Eosinophil 1% Basophils 0% Platelets 210,000 cells/µL ESR 18 mm (1st hour) Urinalysis shows: pH 6.4 Color dark brown RBC plenty WBC 3–4/HPF Protein absent Cast RBC and granular casts Glucose absent Crystal none Ketone absent Nitrite absent Which of the following laboratory findings can be expected in this patient?
A 37-year-old man presents to the emergency department for a persistent fever. The patient states he has felt unwell for the past week and has felt subjectively febrile. The patient has a past medical history of a suicide attempt and alcohol abuse. He is not currently taking any medications. The patient admits to using heroin and cocaine and drinking 5-8 alcoholic drinks per day. His temperature is 103°F (39.4°C), blood pressure is 92/59 mmHg, pulse is 110/min, respirations are 20/min, and oxygen saturation is 96% on room air. Cardiopulmonary exam is notable for a systolic murmur heard best along the left sternal border. Dermatologic exam reveals scarring in the antecubital fossa. Which of the following is the next best step in management?
A 55-year-old male bodybuilder presents to the emergency department with weakness of his right arm. The patient states he has experienced these symptoms for a few weeks; however, today his hand felt so weak he dropped his cup of tea. The patient has a past medical history of diabetes. He drinks 2-7 alcoholic drinks per day and has smoked 2 packs of cigarettes per day since he was 25. The patient admits to using anabolic steroids. He has lost 17 pounds since he last came to the emergency department 1 month ago. His temperature is 99.5°F (37.5°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam reveals decreased sensation in the right arm and 2/5 strength in the right arm and 5/5 strength in the left arm. The patient states that he is experiencing a dull aching and burning pain in his right arm during the exam. Which of the following is the most likely diagnosis?
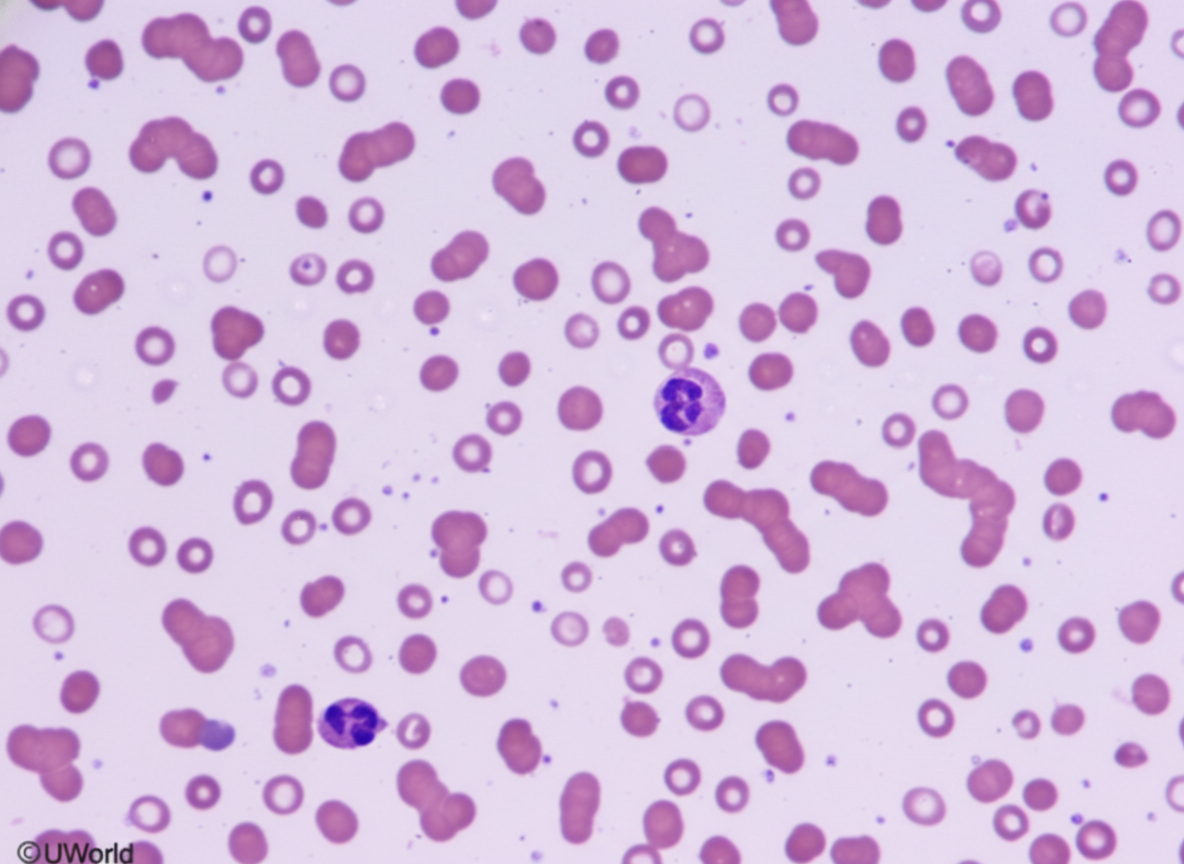
A 69-year-old woman comes to the physician because of a 3-week history of headache and worsening vision. Ophthalmologic examination shows a visual acuity of 20/120 in the right eye and 20/80 in the left eye. Physical examination shows no other abnormalities. Laboratory studies show a hemoglobin of 14.2 g/dL and total serum calcium of 9.9 mg/dL. A photomicrograph of a peripheral blood smear is shown. Serum electrophoresis shows increased concentration of a pentameric immunoglobulin. Which of the following is the most likely diagnosis?
A 70-year-old man is accompanied by his wife to the primary care clinic for hand tremors. He states that he first noticed the tremor of his left hand 1 year ago. Since then, the tremor has been worsening and now he can hardly relax when trying to read. His wife says that she is also worried about his memory. She had to take over the finances several weeks ago after learning that he had forgotten to pay the bills for the past few months. The patient’s medical history is significant for hypertension. He takes aspirin and amlodipine. His mother had schizophrenia. The patient drinks 1-2 beers a night and is a former cigar smoker. On physical examination, he speaks softly and has reduced facial expressions. He has a resting tremor that is worse on the left, and he resists manipulation of his bilateral upper extremities. Which of the following is the most likely diagnosis?
A 69-year-old man presents for a general follow up appointment. He states that he is doing well and wants to be sure he is healthy. The patient’s past medical history is significant for type II diabetes mellitus, peripheral vascular disease, and hypertension. His current medications include metformin, glyburide, lisinopril, metoprolol and hydrochlorothiazide. His blood pressure is 130/90 mmHg and pulse is 80/min. A fasting lipid panel was performed last week demonstrating an LDL of 85 mg/dL and triglycerides of 160 mg/dL. The patient states that he has not experienced any symptoms since his last visit. The patient’s blood glucose at this visit is 100 mg/dL. Which of the following is recommended in this patient?
A 16-year-old boy with a history of severe, persistent asthma presents to the emergency department with severe shortness of breath and cough. He states that he was outside playing basketball with his friends, forgot to take his inhaler, and began to have severe difficulty breathing. On exam, he is in clear respiratory distress with decreased air movement throughout all lung fields. He is immediately treated with beta-agonists which markedly improve his symptoms. Prior to treatment, which of the following was most likely observed in this patient?
A 68-year-old woman is brought to the emergency department by ambulance after she was found down by her daughter. She lives alone in her apartment so it is unclear when she began to develop symptoms. Her medical history is significant for cardiac arrhythmias, diabetes, pericarditis, and a stroke 2 years ago. On presentation her temperature is 98.1°F (36.7°C), blood pressure is 88/51 mmHg, pulse is 137/min, and respirations are 18/min. On physical exam her skin is cold and clammy. If special tests were obtained, they would reveal dramatically decreased pulmonary capillary wedge pressure, increased systemic vascular resistance, and mildly decreased cardiac output. Which of the following treatments would most directly target the cause of this patient's low blood pressure?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app