
Cardiology — MCQs

On this page
A 65-year-old man comes to the physician because of a 10-month history of crampy left lower extremity pain that is exacerbated by walking and relieved by rest. The pain is especially severe when he walks on an incline. He has a 20-year history of type 2 diabetes mellitus, for which he takes metformin. He has smoked 1 pack of cigarettes daily for 40 years. His blood pressure is 140/92 mm Hg. Physical examination shows dry and hairless skin over the left foot. Which of the following is the most likely underlying cause of this patient's symptoms?
A 51-year-old woman with a history of palpitations is being evaluated by a surgeon for epigastric pain. It is discovered that she has an epigastric hernia that needs repair. During her preoperative evaluation, she is ordered to receive lab testing, an electrocardiogram (ECG), and a chest X-ray. These screening studies are unremarkable except for her chest X-ray, which shows a 2 cm isolated pulmonary nodule in the middle lobe of the right lung. The nodule has poorly defined margins, and it shows a dense, irregular pattern of calcification. The patient is immediately referred to a pulmonologist for evaluation of the lesion. The patient denies any recent illnesses and states that she has not traveled outside of the country since she was a child. She has had no sick contacts or respiratory symptoms, and she does not currently take any medications. She does, however, admit to a 20-pack-year history of smoking. Which of the following is the most appropriate next step in evaluating this patient’s diagnosis with regard to the pulmonary nodule?
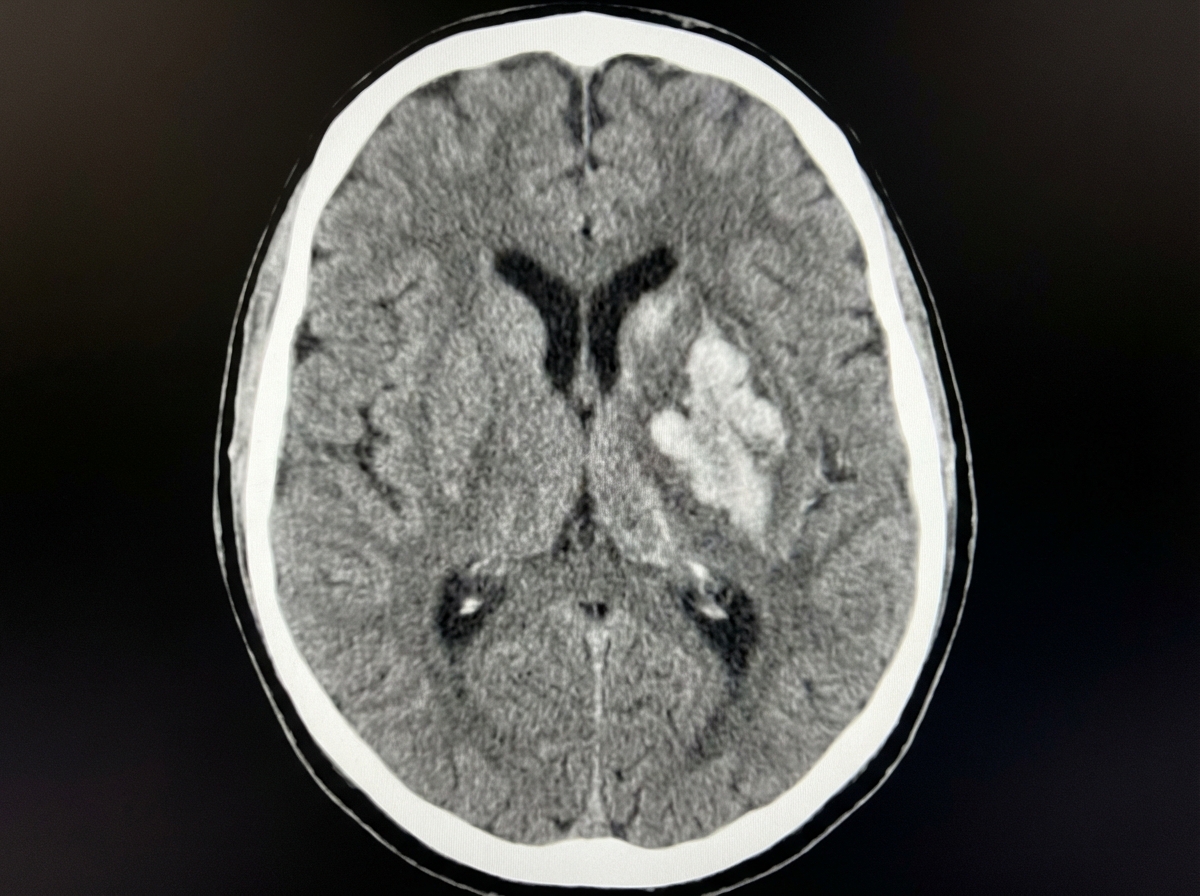
A 68-year-old woman is brought to the emergency department after being found unresponsive in her bedroom in a nursing home facility. Her past medical history is relevant for hypertension, diagnosed 5 years ago, for which she has been prescribed a calcium channel blocker and a thiazide diuretic. Upon admission, she is found with a blood pressure of 200/116 mm Hg, a heart rate of 70/min, a respiratory rate of 15 /min, and a temperature of 36.5°C (97.7°F). Her cardiopulmonary auscultation is unremarkable, except for the identification of a 4th heart sound. Neurological examination reveals the patient is stuporous, with eye-opening response reacting only to pain, no verbal response, and flexion withdrawal to pain. Both pupils are symmetric, with the sluggish pupillary response to light. A noncontrast CT of the head is performed and is shown in the image. Which of the following is the most likely etiology of this patient’s condition?
A 51-year-old woman comes to the physician because of a 3-day history of worsening shortness of breath, nonproductive cough, and sharp substernal chest pain. The chest pain worsens on inspiration and on lying down. The patient was diagnosed with breast cancer 2 months ago and was treated with mastectomy followed by adjuvant radiation therapy. She has hypertension and hyperlipidemia. Current medications include tamoxifen, valsartan, and pitavastatin. She has smoked a pack of cigarettes daily for 15 years but quit after being diagnosed with breast cancer. Her pulse is 95/min, respirations are 20/min, and blood pressure is 110/60 mm Hg. Cardiac examination shows a scratching sound best heard at the left lower sternal border. An ECG shows sinus tachycardia and ST segment elevations in leads I, II, avF, and V1–6. Which of the following is the most likely underlying cause of this patient's symptoms?
A 35-year-old African-American female presents to the emergency room complaining of chest pain. She also complains of recent onset arthritis and increased photosensitivity. Physical examination reveals bilateral facial rash. Which of the following is most likely to be observed in this patient?
A 67-year-old man with a 55-pack-year smoking history, diabetes type II, and hyperlipidemia presents to his primary care clinic for an annual exam. He has no complaints. He reports that his blood glucose has been under tight control and that he has not smoked a cigarette for the past 5 months. His temperature is 97.5°F (36.4°C), blood pressure is 182/112 mmHg, pulse is 85/min, respirations are 15/min, and oxygen saturation is 95% on room air. Physical examination is notable for bruits bilaterally just lateral of midline near his umbilicus. The patient is started on anti-hypertensive medications including a beta-blocker, a thiazide diuretic, and a calcium channel blocker. He returns 1 month later with no change in his blood pressure. Which of the following is the best next step in management?
A 30-year-old African-American woman comes to the physician for a routine checkup. She feels well. She has a history of type 2 diabetes mellitus that is well-controlled with metformin. Her mother died of a progressive lung disease at the age of 50 years. The patient is sexually active with her husband, and they use condoms consistently. She has smoked one pack of cigarettes daily for the past 10 years. She drinks one to two glasses of wine per day. She does not use illicit drugs. Vital signs are within normal limits. Examination, including ophthalmologic evaluation, shows no abnormalities. Laboratory studies, including serum creatinine and calcium concentrations, are within normal limits. An ECG shows no abnormalities. A tuberculin skin test is negative. A chest x-ray is shown. Which of the following is the most appropriate next step in management?

A 67-year-old woman presents with right leg pain and swelling of 5 days’ duration. She has a history of hypertension for 15 years and had a recent hospitalization for pneumonia. She had been recuperating at home but on beginning to mobilize and walk, the right leg became painful and swollen. Her temperature is 37.1°C (98.7°F), the blood pressure is 130/80 mm Hg, and the pulse is 75/min. On physical examination, the right calf is 4 cm greater in circumference than the left when measured 10 cm below the tibial tuberosity. Dilated superficial veins are present on the right foot and the right leg is slightly redder than the left. There is some tenderness on palpation in the popliteal fossa behind the knee. Which of the following is the best initial step in the management of this patient’s condition?
A 66-year-old man comes to the physician because of difficulty walking for the past year. He reports that his gait has become slower and that initiating steps has become more challenging. During the past 6 months, his family has noticed that he is starting to forget important family meetings and holidays. On a number of occasions, he has not been able to get to the bathroom in time in order to urinate. He has hypertension treated with hydrochlorothiazide. His father died of Parkinson's disease at the age of 63 years. The patient had smoked one pack of cigarettes daily for 40 years, but quit 10 years ago. His vital signs are within normal limits. On mental status examination, he is confused and has short-term memory deficits. He has a wide-based, shuffling gait. Muscle strength is normal. Deep tendon reflexes are 2+ bilaterally. An MRI of the head is shown. Which of the following is the most likely underlying cause of this patient's symptoms?

A 67-year-old man presents to his primary care provider because of fatigue and loss of appetite. He is also concerned that his legs are swollen below the knee. He has had type 2 diabetes for 35 years, for which he takes metformin and glyburide. Today his temperature is 36.5°C (97.7°F), the blood pressure is 165/82 mm Hg, and the pulse is 88/min. Presence of which of the following would make diabetic kidney disease less likely in this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app