
Cardiology — MCQs

On this page
A 41-year-old man presents to a New Mexico emergency department with a 12 hour history of shortness of breath and a nonproductive cough. He says that last week he experienced fevers, chills, fatigue, and myalgias but assumed that he simply had a cold. The symptoms went away after 3 days and he felt fine for several days afterward until he started experiencing shortness of breath even at rest. He works as an exterminator and recently had a job in a rodent infested home. Physical exam reveals a thin, tachypneic man with diffuse rales bilaterally. The most likely cause of this patient's symptoms is associated with which of the following?
A 51-year-old woman is brought to the emergency department because of an aggressive cough with copious amounts of thick, foamy, yellow-green sputum. She says she has had this cough for about 11 years with exacerbations similar to her presentation today. She also reports that her cough is worse in the morning. She was evaluated multiple times in the past because of recurrent bouts of bronchitis that have required treatment with antibiotics. She is a non-smoker. On physical examination, the blood pressure is 125/78 mm Hg, pulse rate is 80/min, respiratory rate is 16/min, and temperature is 36.7°C (98.0°F). Chest auscultation reveals crackles and wheezing over the right middle lobe and the rest of her physical examinations are normal. The chest X-ray shows irregular opacities in the right middle lobe and diffuse airway thickening. Based on this history and physical examination, which of the following is the most likely diagnosis?
A 44-year-old woman with recurrent urinary tract infections is brought to the emergency department by ambulance after sudden onset of severe headache 30 minutes ago. She has a history of occasional, mild headaches in the morning. There is no other history of serious illness. Both her father and her paternal grandmother died of chronic kidney disease. Her temperature is 37.2°C (99.1°F) and blood pressure is 145/90 mm Hg. Physical examination shows neck stiffness. When her hip is flexed, she is unable to fully extend her knee because of pain. Lumbar puncture performed 12 hours after headache onset yields 10 mL of yellow-colored fluid with no leukocytes. Which of the following is the most likely predisposing factor for this patient's current condition?
A 72-year-old man presents to the emergency department because of difficulty breathing and sharp chest pain. The chest pain increases in intensity with lying down, and it radiates to the scapular ridge. Approximately 3 weeks ago, he had an anterior ST-elevation myocardial infarction, which was treated with intravenous alteplase. He was discharged home in a stable condition. Current vital signs include a temperature of 38.1 (100.5°F), blood pressure of 131/91 mm Hg, and pulse of 99/min. On examination, heart sounds are distant and a scratching sound is heard on the left sternal border. ECG reveals widespread concave ST elevations in the precordial leads and PR depressions in leads V2-V6. Which of the following is the most likely cause of this patient condition?
A 20-year-old man comes to the emergency room because of palpitations and mild dyspnea for the last 2 hours. He has had similar episodes in the past that resolved within 20 minutes, but they have been worsening since he started training for his first marathon 1 month ago. Ten years ago, he was treated for streptococcal pharyngitis with a 10-day course of penicillin. His maternal uncle passed away unexpectedly from a heart condition at age 40. He is 180 cm (5 ft 11 in) tall and weighs 85 kg (187 lb); BMI is 26.2 kg/m2. His temperature is 36.5°C (97.7°F), pulse is 70/min, respirations are 18/min, and blood pressure is 132/60 mm Hg. On examination, there is a decrescendo early diastolic murmur heard best along the left sternal border. His head slightly bobs about every second. The remainder of the examination shows no abnormalities. Which of the following is most likely to be present?
A 58-year-old man comes to the physician because of intermittent throbbing headaches over the past year. The headaches are worse when he wakes up and are not accompanied by other symptoms. The patient also reports trouble concentrating on daily tasks at work. His wife has been complaining lately about his snoring during sleep, which he attributes to his chronic sinusitis. He has a history of hypertension and an allergy to dust mites. He has smoked a pack of cigarettes daily for 14 years. His pulse is 72/min and blood pressure is 150/95 mm Hg. He is 178 cm (5 ft 10 in) tall and weighs 120 kg (265 lb); BMI is 37.9 kg/m2. Neurological and cutaneous examination shows no abnormalities. Which of the following is the most likely cause of this patient's hypertension?
A 27-year-old man with a past medical history of type I diabetes mellitus presents to the emergency department with altered mental status. The patient was noted as becoming more lethargic and confused over the past day, prompting his roommates to bring him in. His temperature is 99.0°F (37.2°C), blood pressure is 107/68 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Laboratory values are ordered as seen below. Serum: Na+: 144 mEq/L Cl-: 100 mEq/L K+: 6.3 mEq/L HCO3-: 16 mEq/L BUN: 20 mg/dL Glucose: 599 mg/dL Creatinine: 1.4 mg/dL Ca2+: 10.2 mg/dL Which of the following is the appropriate endpoint of treatment for this patient?
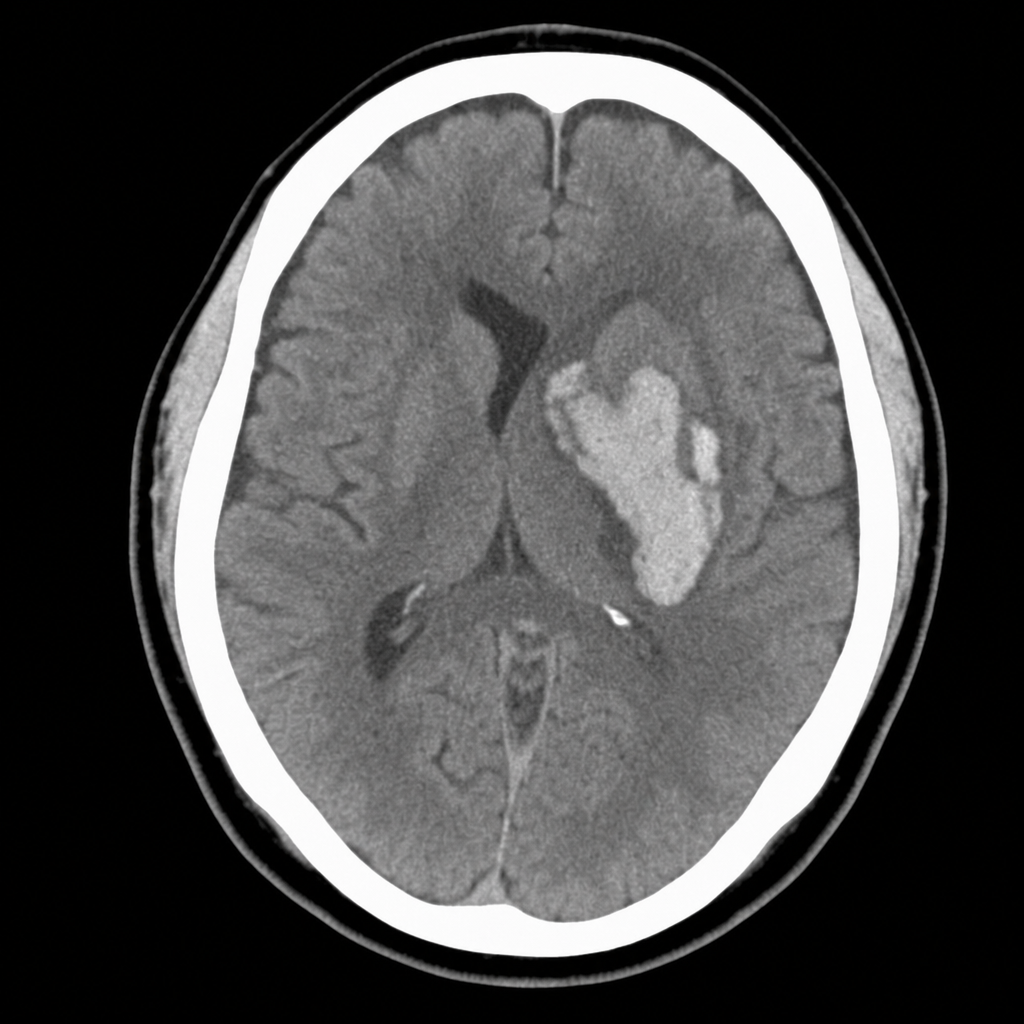
A 59-year-old woman is brought to the emergency department for confusion. She was in her usual state of health until about 2 hours ago when she was found trying to cook a frozen pizza in her medicine cabinet. She also complained to her husband that she had a terrible headache. Her past medical history is notable for hypertension, which has been difficult to control on multiple medications. Her temperature is 37.1°C (98.8°F), the pulse is 75/min, and the blood pressure is 202/128 mm Hg. On physical exam, she is alert and oriented only to self. The physical exam is otherwise unremarkable and the neurologic exam shows no focal neurological deficits. Noncontrast CT head imaging is unremarkable; a T2-weighted image from the patient's MRI brain scan is shown. Which of the following is the next best step in management for this patient?
A 70-year-old man with a 2 year history of Alzheimer disease is brought in from his nursing facility with altered mental status and recurrent falls during the past few days. Current medications include donepezil and galantamine. His vital signs are as follows: temperature 36.0°C (96.8°F), blood pressure 90/60 mm Hg, heart rate 102/min, respiratory rate 22/min. Physical examination reveals several lacerations on his head and extremities. He is oriented only to the person. Urine and blood cultures are positive for E. coli. The patient is admitted and initial treatment with IV fluids, antibiotics, and subcutaneous prophylactic heparin. On the second day of hospitalization, diffuse bleeding from venipuncture sites and wounds is observed. His blood test results show thrombocytopenia, prolonged PT and PTT, and a positive D-dimer. Which of the following is the most appropriate next step in the management of this patient's condition?
A 69-year-old male presents to the emergency department for slurred speech and an inability to use his right arm which occurred while he was eating dinner. The patient arrived at the emergency department within one hour. A CT scan was performed of the head and did not reveal any signs of hemorrhage. The patient is given thrombolytics and is then managed on the neurology floor. Three days later, the patient is recovering and is stable. He seems depressed but is doing well with his symptoms gradually improving as compared to his initial presentation. The patient complains of neck pain that has worsened slowly over the past few days for which he is being given ibuprofen. Laboratory values are ordered and return as indicated below: Serum: Na+: 130 mEq/L K+: 3.7 mEq/L Cl-: 100 mEq/L HCO3-: 24 mEq/L Urea nitrogen: 7 mg/dL Glucose: 70 mg/dL Creatinine: 0.9 mg/dL Ca2+: 9.7 mg/dL Urine: Appearance: dark Glucose: negative WBC: 0/hpf Bacterial: none Na+: 320 mEq/L/24 hours His temperature is 99.5°F (37.5°C), pulse is 95/min, blood pressure is 129/70 mmHg, respirations are 10/min, and oxygen saturation is 98% on room air. Which of the following is the best next step in management?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app