
Cardiology — MCQs

On this page
A 29-year-old man presents to the emergency department with chest pain and fatigue for the past week. The patient is homeless and his medical history is not known. His temperature is 103°F (39.4°C), blood pressure is 97/58 mmHg, pulse is 140/min, respirations are 25/min, and oxygen saturation is 95% on room air. Physical exam is notable for scars in the antecubital fossa and a murmur over the left sternal border. The patient is admitted to the intensive care unit and is treated appropriately. On day 3 of his hospital stay, the patient presents with right-sided weakness in his arm and leg and dysarthric speech. Which of the following is the most likely etiology of his current symptoms?
An otherwise healthy 28-year-old woman comes to the physician because of a 14-day history of painful red nodules on her legs associated with malaise and mild joint pains. She reports that the nodules were initially smaller and distinct but some have fused together over the past 3–4 days and now appear like bruises. There is no preceding history of fever, trauma, or insect bites. Her vital signs are within normal limits. A photograph of the tender lesions on her shins is shown. The remainder of the examination shows no abnormalities. Complete blood count and antistreptolysin O (ASO) titers are within the reference range. Erythrocyte sedimentation rate is 30 mm/h. Which of the following is the most appropriate next step in management ?

A 63-year-old man presents to the clinic with fever accompanied by shortness of breath. The symptoms developed a week ago and have been progressively worsening over the last 2 days. He reports his cough is productive of thick, yellow sputum. He was diagnosed with chronic obstructive pulmonary disease 3 years ago and has been on treatment ever since. He quit smoking 10 years ago but occasionally experiences shortness of breath along with chest tightness that improves with the use of an inhaler. However, this time the symptoms seem to be more severe and unrelenting. His temperature is 38.6°C (101.4°F), the respirations are 21/min, the blood pressure is 100/60 mm Hg, and the pulse is 105/min. Auscultation reveals bilateral crackles and expiratory wheezes. His oxygen saturation is 95% on room air. According to this patient’s history, which of the following should be the next step in the management of this patient?
Please refer to the summary above to answer this question Which of the following is the most likely diagnosis? Patient Information Age: 66 years Gender: M, self-identified Ethnicity: African-American Site of Care: office History Reason for Visit/Chief Concern: "I need to go to the bathroom all the time." History of Present Illness: 1-year history of frequent urination urinates every 2–3 hours during the day and wakes up at least 3 times at night to urinate has had 2 episodes of cystitis treated with antibiotics in the past 4 months has a weak urinary stream has not noticed any blood in the urine does not have any pain with urination or ejaculatory dysfunction Past Medical History: type 2 diabetes mellitus nephrolithiasis, treated with percutaneous nephrolithotomy essential tremor Medications: metformin, canagliflozin, propranolol Allergies: sulfa drugs Social History: sexually active with his wife; does not use condoms consistently has smoked one pack of cigarettes daily for 50 years drinks one to two glasses of beer weekly Physical Examination Temp Pulse Resp BP O2 Sat Ht Wt BMI 37°C (98.6°F) 72/min 16/min 134/81 mm Hg – 183 cm (6 ft) 105 kg (231 lb) 31 kg/m2 Appearance: no acute distress Pulmonary: clear to auscultation Cardiac: regular rate and rhythm; normal S1, S2; S4 gallop Abdominal: overweight; no tenderness, guarding, masses, bruits, or hepatosplenomegaly Extremities: no joint erythema, edema, or warmth; dorsalis pedis, radial, and femoral pulses intact Genitourinary: no lesions or discharge Rectal: slightly enlarged, smooth, nontender prostate Neurologic: alert and oriented; cranial nerves grossly intact; no focal neurologic deficits
A 53-year-old woman comes to the physician because of intermittent heaviness and paresthesia of the right arm for the past 2 months. She has also had multiple episodes of lightheadedness while painting a mural for the past 2 weeks. During these episodes, she was nauseated and had blurred vision. Her symptoms resolved after she drank some juice. She has hypertension, type 2 diabetes mellitus, and hypercholesterolemia. Current medications include metformin, glipizide, enalapril, and atorvastatin. She appears anxious. Examination shows decreased radial and brachial pulses on the right upper extremity. The skin over the right upper extremity is cooler than the left. Cardiopulmonary examination shows no abnormalities. Neurologic examination shows no focal findings. Which of the following is the most likely underlying cause of this patient's symptoms?
A 33-year-old woman presents to the emergency department with weakness. She states that at the end of the day she feels so fatigued and weak that she can hardly care for herself. She currently feels this way. The patient has had multiple illnesses recently and has been traveling, hiking, and camping. Her temperature is 98.0°F (36.7°C), blood pressure is 124/84 mmHg, pulse is 82/min, respirations are 12/min, and oxygen saturation is 98% on room air. Physical exam is notable for 2/5 strength of the upper extremities and 4/5 strength of the lower extremities. Visual exam is notable for mild diplopia. Which of the following is the most likely diagnosis?
A 32-year-old male presents for a new patient visit. He states that he is in good health but has had decreasing exercise tolerance and increased levels of shortness of breath over the past 5 years. He believed that it was due to aging; he has not seen a doctor in 10 years. On auscultation, you note an early diastolic decrescendo blowing murmur that radiates along the left sternal border. In the United States, what is the most likely cause of this patient's condition?
A 45 year-old gentleman presents to his primary care physician complaining of wrist pain and is diagnosed with carpal tunnel syndrome. Upon further questioning, the patient admits that he has recently been outgrowing his gloves and shoes and has had to purchase a new hat as well due to increased head size. Upon exam, he is found to have new mild hypertension and on basic labs he is found to be hyperglycemic. Which of the following is the best blood test to diagnose his suspected disorder?
A 59-year-old male with a history of hypertension presents with chest pain and hoarseness. Patient reports that his hoarseness onset gradually approximately 2 weeks ago and has steadily worsened. He states that approximately 2 hours ago he had sudden onset chest pain which has not improved. The patient describes the chest pain as severe, sharp in character, localized to the midline and radiating to the back. Past medical history is significant for hypertension diagnosed 10 years previously, which was being managed medically, although patient admits he stopped taking his medication and has not been to his doctor in the last couple of years. No current medications. Patient admits to a 20-pack-year smoking history. Vital signs are temperature 37 °C (98.6 °F), blood pressure 169/100 mm Hg, pulse 85/min, respiration rate 19/min, and oxygen saturation 98% on room air. On physical exam, patient is diaphoretic and in distress. Cardiac exam is significant for an early diastolic murmur. Lungs are clear to auscultation. Remainder of physical exam is normal. While performing the exam, the patient suddenly grips his chest and has a syncopal episode. He cannot be roused. Repeat vital signs show blood pressure 85/50 mm Hg, pulse 145/min, respiration rate 25/min, and oxygen saturation 92% on room air. Extremities are pale and cool. Patient is intubated. High flow supplemental oxygen and aggressive fluid resuscitation are initiated. Type and crossmatch are ordered. Which of the following is the next best step in management?
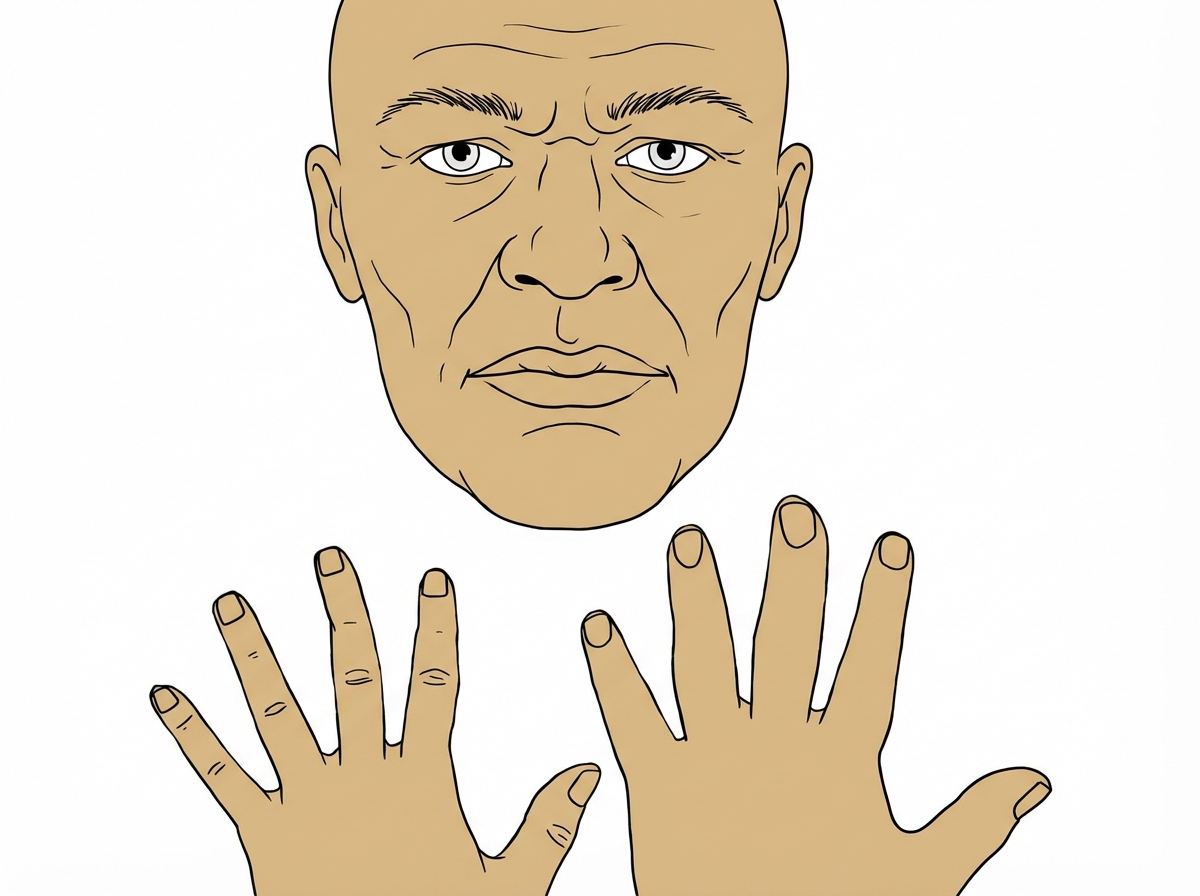
A 43-year-old man visits his physician’s office for a routine check-up. He tells his physician that he is otherwise healthy, except for persistent headaches that he gets every morning. Upon further questioning, he reveals that he has been changing glove sizes quite frequently over the past couple of years. His wedding ring doesn’t fit him anymore. He thought this was probably due to some extra weight that he has put on. Vital signs include: blood pressure 160/90 mm Hg, heart rate 82/min, and respiratory rate 21/min. His current physical appearance is cataloged in the image. His past medical history is significant for diabetes for which he has been receiving treatment for the past 2 years. Which of the following organs most likely has a structural abnormality that has resulted in this patient’s current presentation?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app