
Cardiology — MCQs

On this page
A 30-year-old woman is brought to the clinic at her husband's insistence for sleep disturbances. Most nights of the week she repeatedly gets out of bed to pace around their apartment before returning to bed. The woman says that while she's lying in bed, she becomes overwhelmed by a "creepy-crawly" feeling in her legs that she can only relieve by getting out of bed. Past medical history is noncontributory and physical exam is unremarkable. Which of the following laboratory studies is most likely abnormal in this patient?
A 70-year-old male with a 10-year history of COPD visits his pulmonologist for a checkup. Physical examination reveals cyanosis, digital clubbing, and bilateral lung wheezes are heard upon auscultation. The patient has a cough productive of thick yellow sputum. Which of the following findings is most likely present in this patient?
A 57-year-old woman is admitted to the intensive care unit for management of shock. Her pulse is feeble and blood pressure is 86/45 mm Hg. The patient undergoes pulmonary artery catheterization which shows an elevated pulmonary capillary wedge pressure and increased systemic vascular resistance. Which of the following additional findings is most likely in this patient?
A 72-year-old man presents to the emergency department with severe respiratory distress. He was diagnosed with metastatic pancreatic cancer 6 months ago and underwent 2 rounds of chemotherapy. He says that he has had a cough and flu-like symptoms for the past week. During the interview, he is having progressive difficulty answering questions and suddenly becomes obtunded with decreased motor reflexes. His temperature is 38.8°C (102.0°F), blood pressure is 90/60 mm Hg, pulse is 94/min, and respirations are 22/min. Pulse oximetry is 82% on room air. The patient’s medical record contains an advanced directive stating that he would like all interventions except for cardiopulmonary resuscitation. Which of the following is the most appropriate next step in management?
A 74-year-old man is brought from a nursing home to the emergency room for progressive confusion. The patient has a history of stroke 3 years ago, which rendered him wheelchair-bound. He was recently started on clozapine for schizoaffective disorder. Vital signs reveal a temperature of 38.7°C (101.66°F), a blood pressure of 100/72 mm Hg, and a pulse of 105/minute. On physical examination, he is disoriented to place and time. Initial lab work-up results are shown: Serum glucose: 945 mg/dL Serum sodium: 120 mEq/L Serum urea: 58 mg/dL Serum creatinine: 2.2 mg/dL Serum osmolality: 338 mOsm/kg Serum beta-hydroxybutyrate: negative Urinalysis reveals: numerous white blood cells and trace ketones Which of the following manifestations is more likely to be present in this patient?
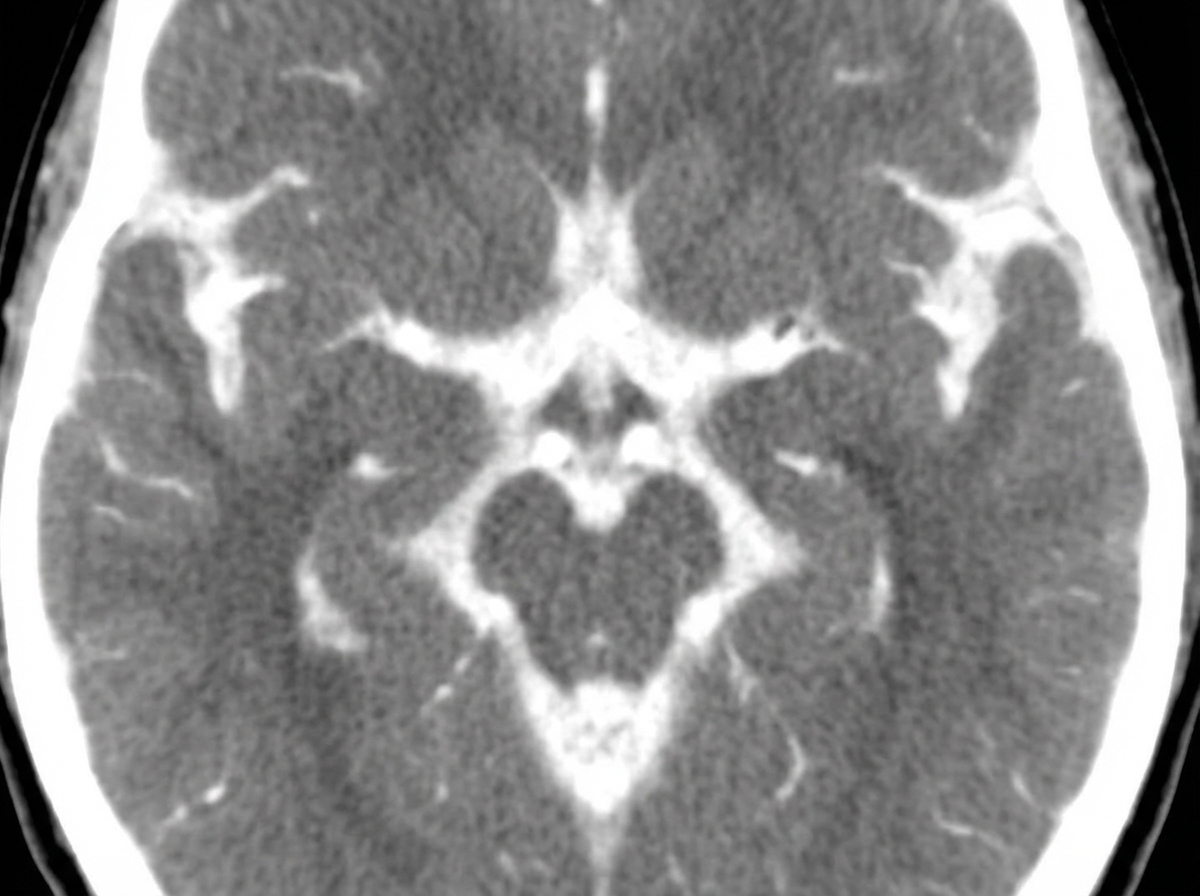
A 32-year-old woman presents with a severe headache and neck pain for the past 60 minutes. She says the headache was severe and onset suddenly like a 'thunderclap'. She reports associated nausea, vomiting, neck pain, and stiffness. She denies any recent head trauma, loss of consciousness, visual disturbances, or focal neurologic deficits. Her past medical history is significant for hypertension, managed with hydrochlorothiazide. She denies any history of smoking, alcohol use, or recreational drug use. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 165/95 mm Hg, pulse 92/min, and respiratory rate 15/min. On physical examination, there is mild nuchal rigidity noted with limited flexion at the neck. A noncontrast computed tomography (CT) scan of the head is performed and shown in the exhibit (see image), demonstrating subarachnoid hemorrhage. Which of the following intravenous antihypertensive agents is the most appropriate next step in the management of this patient's elevated blood pressure?
A 58-year-old woman is followed in the nephrology clinic for longstanding chronic kidney disease (CKD) secondary to uncontrolled hypertension. Her glomerular filtration rate (GFR) continues to decline, and she is approaching initiation of hemodialysis. Plans are made to obtain vascular access at the appropriate time, and the patient undergoes the requisite screening to be enrolled as an end stage renal disease (ESRD) patient. Among patients on chronic hemodialysis, which of the following is the most common cause of death?
A 67-year-old man presents with an excruciatingly painful tongue lesion. He says the lesion was preceded by an intermittent headache for the past month that localized unilaterally to the left temple and occasionally radiates to the right eye. The tongue lesion onset acutely and has been present for a few days. The pain is constant. His past medical history is relevant for hypertension and recurrent migraines. Current medications include captopril. On physical examination, multiple knot-like swellings are seen on the left temple. Findings from an inspection of the oral cavity are shown in the exhibit (see image). Laboratory findings are significant for the following: Hemoglobin 12.9 g/dL Hematocrit 40.7% Leukocyte count 5500/mm3 Neutrophils 65% Lymphocytes 30% Monocytes 5% Mean corpuscular volume 88.2 μm3 Platelet count 190,000/mm3 Erythrocyte sedimentation rate 45 mm/h Which of the following is the next best step in the management of this patient?

A 67-year-old man presents to his primary care physician for a wellness checkup. The patient states he has been doing well and currently has no concerns. The patient's daughter states that she feels he is abnormally fatigued and has complained of light-headedness whenever he gardens. He also admits that he fainted once. The patient has a past medical history of type II diabetes, hypertension, and constipation. He recently had a "throat cold" that he recovered from with rest and fluids. His temperature is 98.9°F (37.2°C), blood pressure is 167/98 mmHg, pulse is 90/min, respirations are 12/min, and oxygen saturation is 99% on room air. Physical exam reveals a systolic murmur heard best along the right upper sternal border. An ECG is performed and demonstrates no signs of ST elevation. Cardiac troponins are negative. Which of the following is the most likely diagnosis?
A 25-year-old man presents to the emergency department for a fever and abdominal pain. The patient states that his pain has been worsening over the past week in the setting of a fever. He has a past medical history of IV drug abuse and multiple admissions for septic shock. His temperature is 102°F (38.9°C), blood pressure is 94/54 mmHg, pulse is 133/min, respirations are 22/min, and oxygen saturation is 100% on room air. Physical exam is notable for a murmur over the left upper sternal border. Abdominal exam reveals left upper quadrant tenderness. Laboratory values are ordered as seen below. Hemoglobin: 15 g/dL Hematocrit: 44% Leukocyte count: 16,700/mm^3 Platelet count: 299,000/mm^3 Which of the following is the most likely diagnosis?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app