
Cardiology — MCQs

On this page
A 15-year-old girl presents with four days of malaise, painful joints, nodular swelling over her elbows, low-grade fever, and a rash on her chest and left shoulder. Two weeks ago, she complained of a sore throat that gradually improved but was not worked up. She was seen for a follow-up approximately one week later. At this visit her cardiac exam was notable for a late diastolic murmur heard best at the apex in the left lateral decubitus position with no radiation. Which of the following is the best step in the management of this patient?
A 30-year-old man comes to the emergency department because of a painful rash for 2 days. The rash initially appeared on his left lower abdomen and has spread to the rest of the abdomen and left upper thigh over the last 24 hours. Pain is exacerbated with movement. He initially thought the skin rash was an allergic reaction to a new laundry detergent, but it did not respond to over-the-counter antihistamines. Six weeks ago, the patient was diagnosed with Hodgkin's lymphoma and was started on doxorubicin, bleomycin, vinblastine, and dacarbazine. He is sexually active with one female partner and uses condoms for contraception. His temperature is 37.9°C (100.2°F), pulse is 80/min, and blood pressure is 117/72 mm Hg. Examination shows two markedly enlarged cervical lymph nodes. A photograph of the rash is shown. Which of the following is the most appropriate next step in management?

A 16-year-old boy comes to the physician with a 4-day history of sore throat and mild fever. He is on the varsity soccer team at his high school, but has been unable to go to practice for the last few days because he has been very tired and is easily exhausted. He has no history of serious illness and takes no medications. His mother has type 2 diabetes mellitus. He appears weak and lethargic. His temperature is 38.7°C (101.7°F), pulse is 84/min, and blood pressure is 116/78 mm Hg. Examination shows enlarged, erythematous, and exudative tonsils; posterior cervical lymphadenopathy is present. Abdominal examination shows no abnormalities. His hemoglobin concentration is 14.5 g/dL and leukocyte count is 11,200/mm3 with 48% lymphocytes. A heterophile antibody test is positive. In addition to supportive therapy, which of the following is the most appropriate next step in management?
A 36-year-old man presents to his physician with the complaint of bilateral lower back pain. The pain is 5/10, constant, aching, aggravated by bending forward and lying supine, and is alleviated by resting in a neutral position. The pain appeared 3 days ago after the patient overstrained at the gym. He does not report changes in sensation or limb weakness. The patient works as a business analyst. The patient’s weight is 88 kg (194 lb), and the height is 186 cm (6 ft 1 in). The vital signs are within normal limits. The neurological examination shows equally normal lower limb reflexes, and preserved muscle tone and power. The paravertebral palpation of the lumbar region increases the pain. Which of the following non-pharmacological interventions is the most appropriate in the presented case?
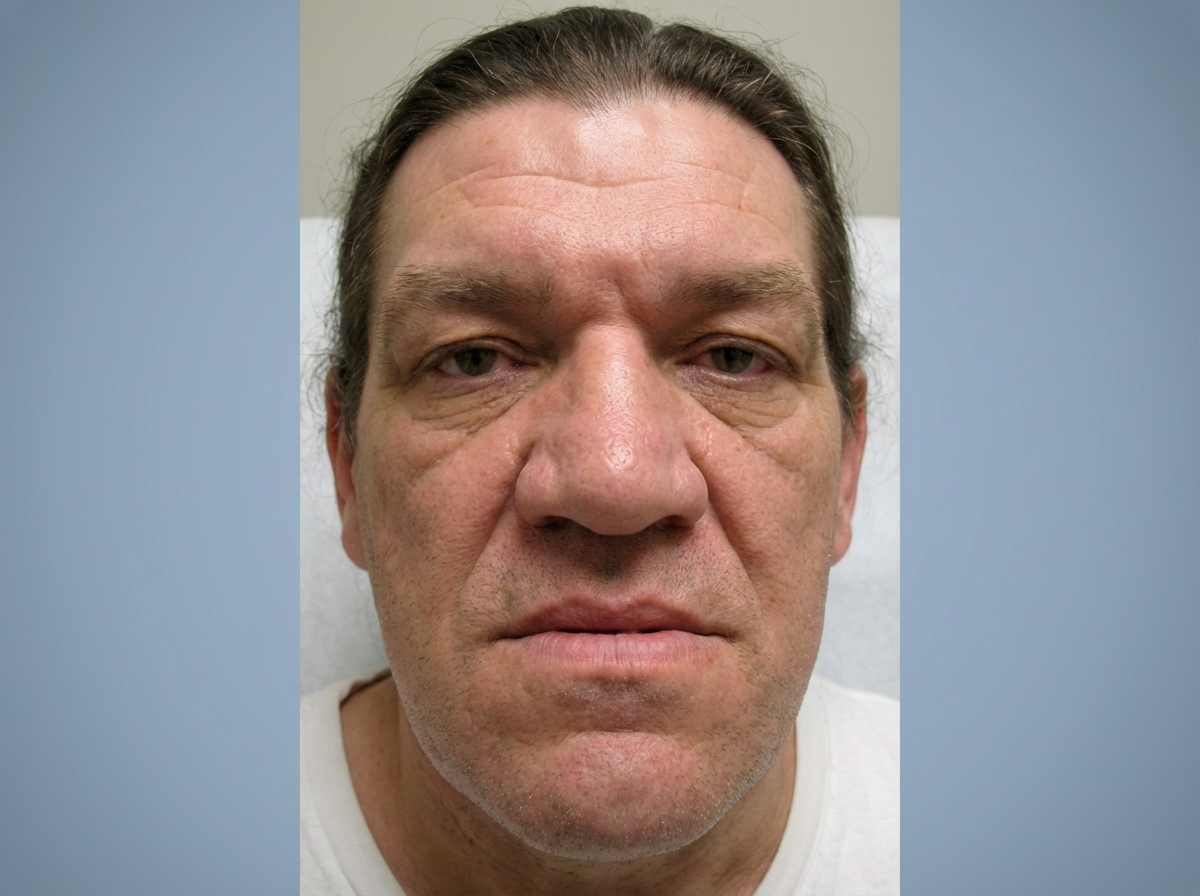
A 46-year-old man comes to the physician for a routine health maintenance examination. He feels well. He has a history of seizures controlled with levetiracetam. He has needed glasses for the past 13 years. His father died of pancreatic cancer. He is 175 cm (5 ft 9 in) tall and weighs 79 kg (174 lbs); BMI is 25.8 kg/m2. Vital signs are within normal limits. A photograph of the face is shown. This patient is most likely to be at increased risk for which of the following conditions?
A 68-year-old man comes to the physician for a routine health maintenance examination. His wife has noticed that his left eye looks smaller than his right eye. He has had left shoulder and arm pain for 3 months. He has hypertension and coronary artery disease. Current medications include enalapril, metoprolol, aspirin, and atorvastatin. His medical history is significant for gonorrhea, for which he was treated in his 30's. He has smoked two packs of cigarettes daily for 35 years. He does not drink alcohol. His temperature is 37°C (98.6°F), pulse is 71/min, and blood pressure is 126/84 mm Hg. The pupils are unequal; when measured in dim light, the left pupil is 3 mm and the right pupil is 5 mm. There is drooping of the left eyelid. The remainder of the examination shows no abnormalities. Application of apraclonidine drops in both eyes results in a left pupil size of 5 mm and a right pupil size of 4 mm. Which of the following is the most appropriate next step in management?
A 30-year-old African American man comes to the doctor's office for an annual checkup. He feels healthy and his only concern is an occasional headache after work. Past medical history is significant for an appendectomy 10 years ago and a fractured arm playing football in high school. His mother has type 2 diabetes mellitus, while his father and grandfather both have hypertension. He does not drink alcohol, smoke cigarettes, or use drugs. His vital signs include: pulse 78/min and regular, respiratory rate 16/min, and temperature 36.8°C (98.2°F). Physical examination reveals an overweight African American man 167 cm (5 ft 6 in) tall and weighing 80 kg (176 lb) with a protuberant belly. BMI is 28.7 kg/m2. The remainder of the examination is unremarkable. During his last 2 visits, his blood pressure readings have been 140/86 mm Hg and 136/82 mm Hg. Today his blood pressure is 136/86 mm Hg and his laboratory tests show: Serum Glucose (fasting) 90.0 mg/dL Serum Electrolytes: Sodium 142.0 mEq/L Potassium 3.9 mEq/L Chloride 101.0 mEq/L Serum Creatinine 0.8 mg/dL Blood urea nitrogen 9.0 mg/dL Urinalysis: Glucose Negative Ketones Negative Leukocytes Negative Nitrite Negative RBCs Negative Casts Negative Which of the following is the next best step in the management of this patient?
A 72-year-old woman is brought to the emergency department by her daughter because of left-sided weakness for 1 hour. She does not have headache or blurring of vision. She has hypertension, hypercholesterolemia, type 2 diabetes, and coronary artery disease. She has smoked one half-pack of cigarettes daily for 45 years. Her medications include atorvastatin, amlodipine, metformin, and aspirin. Her temperature is 37°C (98.6°F), pulse is 92/min, and blood pressure is 168/90 mm Hg. Examination shows a left facial droop. Muscle strength is decreased on the left side. Deep tendon reflexes are 3+ on the left. Sensation to pinprick, light touch, and vibration as well as two-point discrimination are normal. Which of the following is the most likely cause of these findings?
A 69-year-old man is brought to the emergency department for severe tearing lower back pain for 12 hours. The pain radiates to the flank and he describes it as 8 out of 10 in intensity. He has nausea and has vomited several times. He has no fever, diarrhea, or urinary symptoms. When he stands up suddenly, he becomes light-headed and has to steady himself for approximately 1 to 2 minutes before he is able to walk. He has hypertension and hyperlipidemia. Two years ago, he had a myocardial infarction and underwent coronary artery bypass grafting of his right coronary artery. He has smoked one and a half packs of cigarettes daily for 40 years and drinks 1 to 2 beers daily. His current medications include chlorthalidone, atorvastatin, lisinopril, and aspirin. He appears acutely ill. His temperature is 37.2°C (98.9°F), pulse is 130/min and regular, respirations are 35/min, and blood pressure is 80/55 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 85%. Examination shows a pulsatile mass in the abdomen. Intravenous fluids and high-flow oxygen are started. Thirty minutes later, the patient dies. Which of the following was the strongest predisposing factor for the condition leading to this patient's death?
A 19-year-old woman comes to the physician for a routine health maintenance examination. She appears well. Her vital signs are within normal limits. Cardiac auscultation shows a mid-systolic click and a grade 3/6, late-systolic, crescendo murmur that is best heard at the cardiac apex in the left lateral recumbent position. After the patient stands up suddenly, the click is heard during early systole and the intensity of the murmur increases. Which of the following is the most likely underlying cause of this patient's examination findings?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app