
Cardiology — MCQs

On this page
A 36-year-old man presents to his physician with an acute burning retrosternal sensation with radiation to his jaw. This sensation began 20 minutes ago when the patient was exercising at the gym. It does not change with position or with a cough. The patient’s vital signs include: blood pressure is 140/90 mm Hg, heart rate is 84/min, respiratory rate is 14/min, and temperature is 36.6℃ (97.9℉). Physical examination is only remarkable for paleness and perspiration. The patient is given sublingual nitroglycerin, the blood is drawn for an express troponin test, and an ECG is going to be performed. At the moment of performing ECG, the patient’s symptoms are gone. ECG shows increased R amplitude in I, II V3-V6, and ST depression measuring for 0.5 mm in the same leads. The express test for troponin is negative. Which of the following tests would be reasonable to perform next to confirm a diagnosis in this patient?
A 46-year-old woman complains of chronic cough for the past 3 weeks. She was recently diagnosed with hypertension and placed on an angiotensin receptor blocker therapy (ARBs). Chest X-ray shows large nodular densities bilaterally. Bronchial biopsy showed granulomatous inflammation of the pulmonary artery. Lab investigations showed a positive cANCA with a serum creatinine of 3.6 mg/dL. Urine analysis shows RBC casts and hematuria. Which is the most likely cause of this presentation?
A 67-year-old man presents to your office with a chief complaint of constipation and many other perturbing minor medical concerns. He reports tiring easily, which he attributes to old age and years of persistent pain in his back and ribs. A complete blood count shows low hemoglobin and elevated serum creatinine. A peripheral blood smear shows stacks of red blood cells among other findings, and serum electropheresis reveals an abnormal concentration of protein resulting in a spike. Which of the following additional findings would you expect to see in this patient?
A 75-year-old man presents to the physician with difficulty breathing for the last 2 months. He denies any cough, fever, or chest pain. His past medical history is significant for hypertension for which he takes chlorothiazide. He has worked in the construction industry, applying insulation to roofs for over 20 years. He denies smoking, drinking, and illicit drug use. His pulse rate is 74/min, respiratory rate is 14/min, blood pressure is 130/76 mm Hg, and temperature is 36.8°C (98.2°F). Physical examination reveals some end-inspiratory crackles at the lung bases. No other examination findings are significant. The lung inflation curve is obtained for the patient and is shown in the image. Which of the following most likely accounts for this patient's symptoms?

A 55-year-old woman presents to a primary care clinic for a physical evaluation. She works as a software engineer, travels frequently, is married with 2 kids, and drinks alcohol occasionally. She does not exercise regularly. She currently does not take any medications except for occasional ibuprofen or acetaminophen. She is currently undergoing menopause. Her initial vital signs reveal that her blood pressure is 140/95 mmHg and heart rate is 75/min. She weighs 65 kg (143 lb) and is 160 cm (63 in) tall. Her physical exam is unremarkable. A repeat measurement of her blood pressure is the same as before. Among various laboratory tests for hypertension evaluation, the physician requests fasting glucose and hemoglobin A1c levels. Which of the following is the greatest risk factor for type 2 diabetes mellitus?
A 65-year-old man comes to the physician because of a 10-day history of episodic retrosternal pain, shortness of breath, and palpitations. The episodes occur when he climbs stairs or tries to walk briskly on his treadmill. The symptoms resolve when he stops walking. The previous evening he felt dizzy and weak during such an episode. He also reports that he had a cold 2 weeks ago. He was diagnosed with type 2 diabetes mellitus four years ago but is otherwise healthy. His only medication is glyburide. He appears well. His pulse is 62/min and is weak, respirations are 20/min, and blood pressure is 134/90 mmHg. Cardiovascular examination shows a late systolic ejection murmur that is best heard in the second right intercostal space. The lungs are clear to auscultation. Which of the following mechanisms is the most likely cause of this patient's current condition?
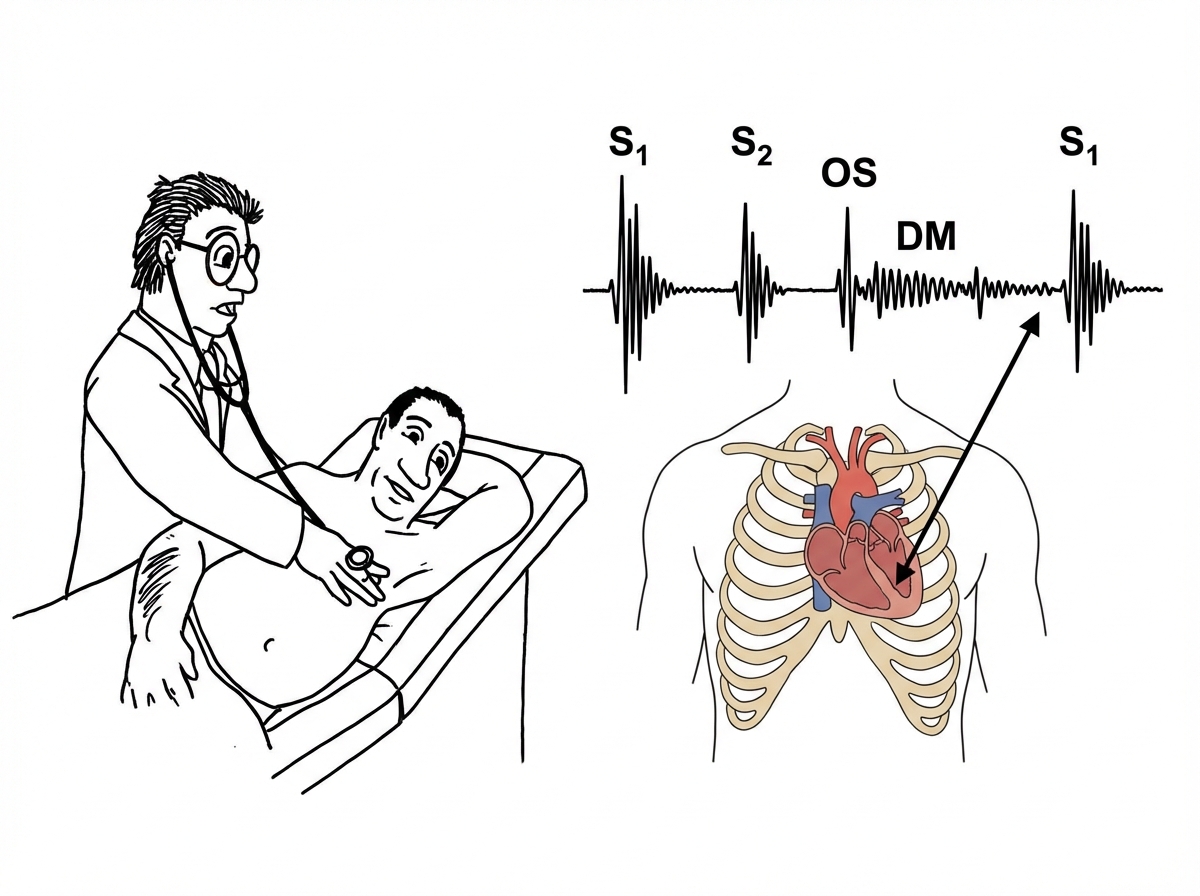
A 48-year-old man comes to the physician because of worsening shortness of breath and nocturnal cough for the past 2 weeks. On two occasions, his cough was bloody. He had a heart condition as a child that was treated with antibiotics. He emigrated to the US from Kazakhstan 15 years ago. Pulmonary examination shows crackles at both lung bases. Cardiac examination is shown. Which of the following is the most likely diagnosis?
A 68-year-old man is brought to the emergency department because of progressive weakness of his lower extremities and urinary incontinence for the past 2 weeks. Over the past 2 months, he has had increasing back pain. His temperature is 37.1°C (98.8°F), pulse is 88/min, and blood pressure is 106/60 mm Hg. Examination shows an ataxic gait. Muscle strength is decreased in bilateral lower extremities. Sensation to pain, temperature, and position sense is absent in the buttocks, perineum, and lower extremities. Ankle clonus is present. Digital rectal examination is unremarkable. An x-ray of the spine shows multiple sclerotic lesions in the thoracic and lumbar vertebrae. Further evaluation of this patient is most likely to show which of the following?
A 47-year-old woman presents to her primary care physician for a wellness checkup. The patient states that she currently feels well and has no complaints. She has failed multiple times at attempting to quit smoking and has a 40 pack-year smoking history. She drinks 4 alcoholic beverages every night. The patient is currently taking a multivitamin and vitamin D supplements. She has also attempted to eat more salmon given that she has heard of its health benefits. Physical exam is notable for back stiffness on mobility testing. The patient states that she frequently has back pain when sitting. Laboratory values are obtained as seen below. Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 1.1 mg/dL Ca2+: 12.2 mg/dL PTH: 75 pg/mL (normal 10 - 65 pg/mL) Urine: Color: Yellow pH: 7.0 Blood: 1+ Protein: Negative Nitrite: Positive Bacteria: Positive Ca2+: Low Benzodiazepines: Positive Which of the following is the best explanation for this patient’s electrolyte abnormalities?
An 82-year-old man—a retired physics professor—presents with progressive difficulty walking. He has bilateral knee osteoarthritis and has used a walker for the past several years. For the past 6 months, he has experienced problems walking and maintaining balance and has been wheelchair-bound. He has fallen several times, hitting his head a few times but never losing consciousness. He complains of occasional difficulty remembering names and phone numbers, but his memory is otherwise fine. He also complains of occasional incontinence. Physical examination reveals a slow wide-based gait with small steps and intermittent hesitation. He scores 22 out of 30 on the Mini-Mental State Examination (MMSE). A brain MRI demonstrates dilated ventricles with high periventricular fluid-attenuated inversion recovery (FLAIR) signal. A large-volume lumbar puncture improves his gait. Which of the following is the most likely risk factor for the development of this condition?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app