
Cardiology — MCQs

On this page
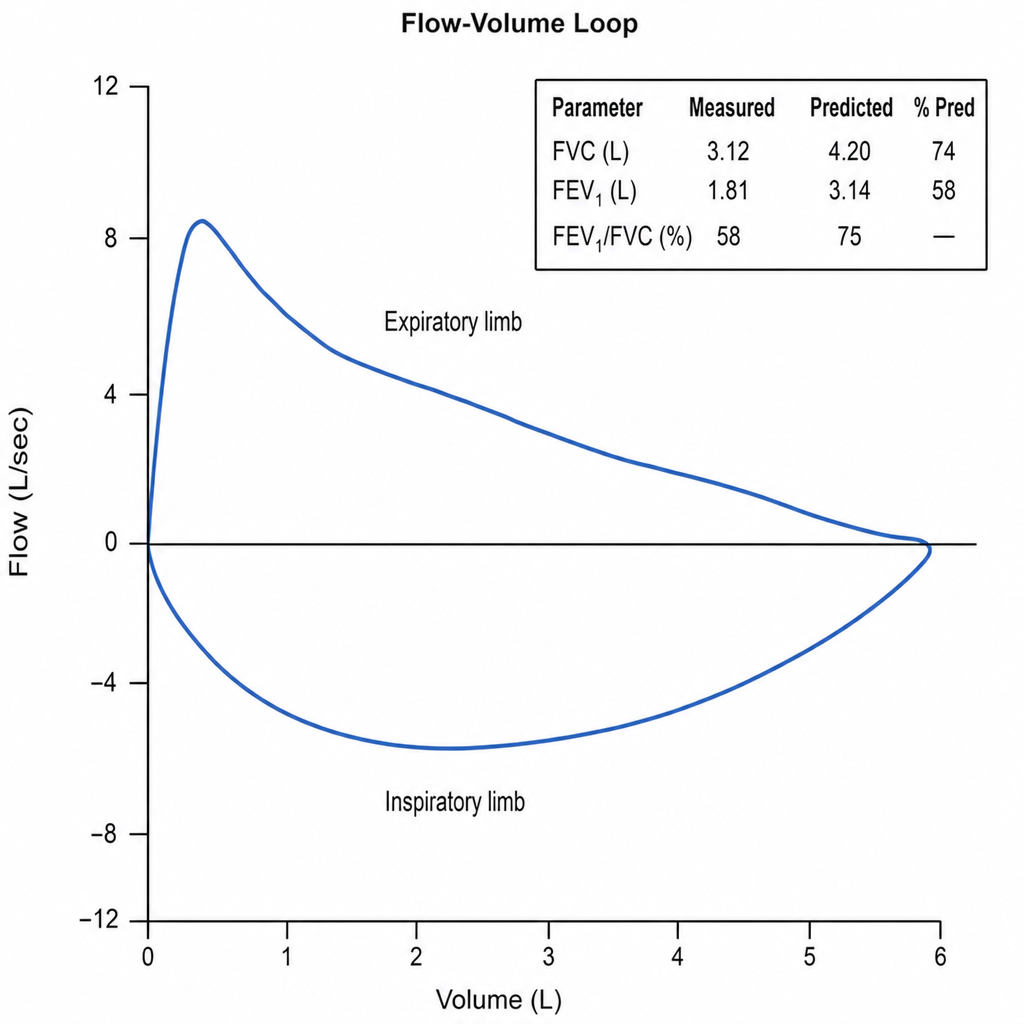
A 61-year-old man with a 45-pack-year smoking history presents with a 4-month history of progressive exertional dyspnea and a productive cough. He has no fever, hemoptysis, or weight loss. Spirometry is performed. Post-bronchodilator FEV1/FVC ratio is 0.58, and FEV1 is 52% of predicted. Lung volumes show a TLC of 128% predicted and RV of 185% predicted. Which of the following additional findings would most strongly support the underlying diagnosis over a restrictive pattern?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app