
Abdominal and Pelvic Radiology — MCQs

On this page
The initial imaging investigation for suspected intestinal obstruction is?
A 70-year-old male presents with a pulsatile abdominal mass. Which diagnostic study is most appropriate to confirm the presence of an abdominal aortic aneurysm?
Which imaging technique is essential for evaluating a suspected perforation of the gastrointestinal tract?
A patient with fever, back pain, and difficulty walking is diagnosed with a psoas abscess. Which imaging modality is the most effective for confirming the diagnosis?
A 60-year-old male with a history of smoking presents with severe abdominal pain and a pulsatile abdominal mass. What is the most appropriate next step in managing this patient?
What does the 'football sign' on an abdominal X-ray indicate?
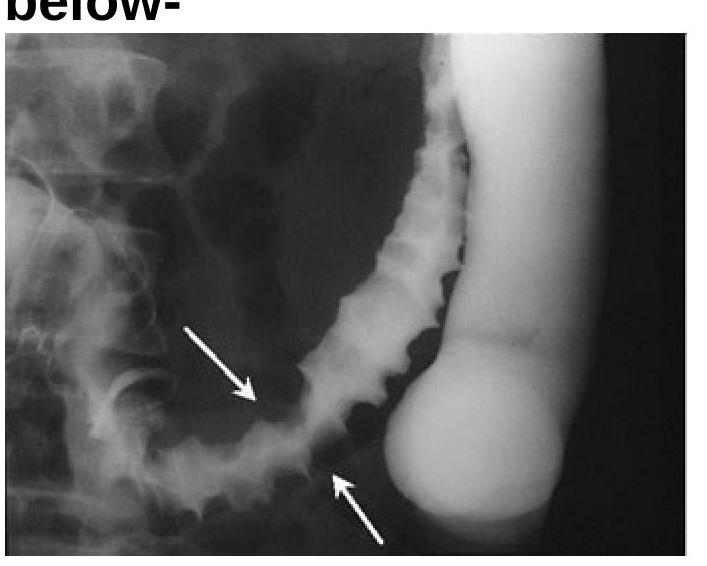
Identify the radiological sign of Ischemic colitis from the image provided.
Chain of lakes appearance is seen in?
Which condition is associated with the "Drooping lily sign"?
Which of the following is a valid imaging criterion for unresectable carcinoma of the pancreas?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app