
Abdominal and Pelvic Radiology — MCQs

On this page
Which of the following findings is NOT associated with carcinoma of the esophagus?
String of beads sign is seen in:
Which of the following conditions is associated with the "Rim sign" in a nephrogram?
What is the primary imaging modality used for diagnosing urethral trauma?
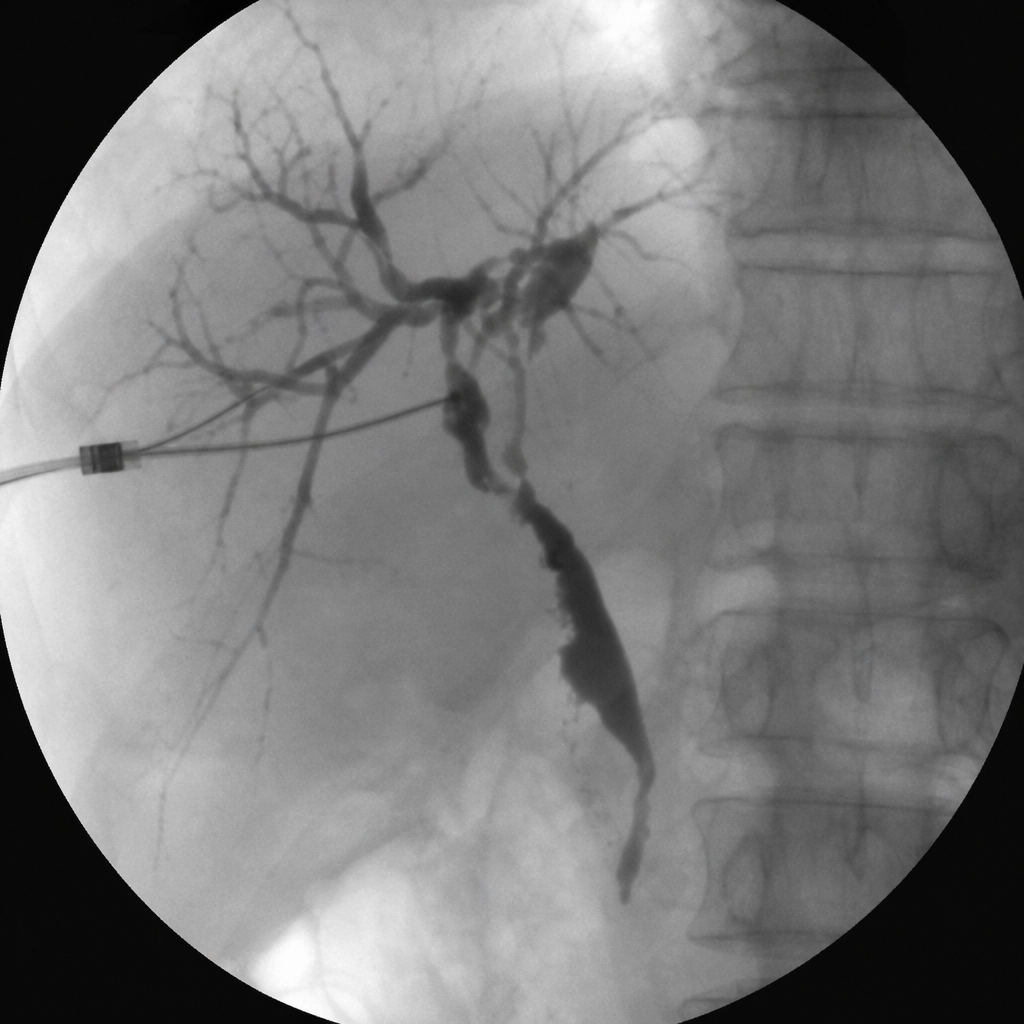
What is the most likely diagnosis in a jaundiced patient with an AP view from a percutaneous transhepatic cholangiogram? (Refer to the image)
A 30-year-old female patient presents with nonprogressive dysphagia for both solids and liquids. The characteristic finding on barium swallow that will confirm the probable diagnosis is:
A 46-year-old chronic diabetic presents to the emergency department with high-grade fever and dysuria. Urine analysis reveals multiple leukocytes and glycosuria. A CT scan of the abdomen shows the following image. What is the most likely diagnosis?

In the context of abdominal imaging, which condition is associated with the 'Claw sign'?
Which of the following statements about hepatocellular carcinoma (HCC) is true? 1. On CECT, rapid wash-in and washout of contrast are seen in HCC. 2. HCC is the most common primary malignant tumor of the liver. 3. LI-RADS provides an algorithm for the diagnosis of HCC. 4. Fibrolamellar HCC has a better prognosis than classic HCC. 5. Alpha-fetoprotein is raised in 50-60% of HCC cases.
Which of the following is characterized by a "cobra head deformity"?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app