
Renal Pathology — MCQs

On this page
Nephrocalcinosis is seen in which of the following conditions?
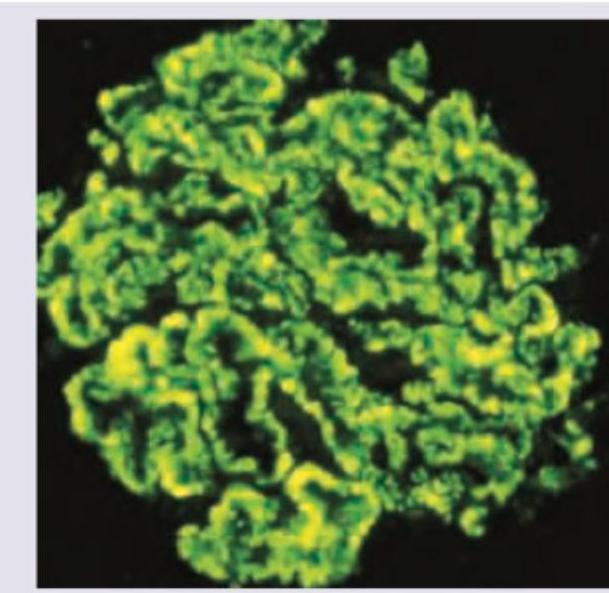
Which is usually a presentation of the condition shown in the immunofluorescence study of the kidney?
Heroin abuse is associated with which type of glomerulonephritis?
Renal biopsy demonstrates concentric, laminated thickening of arteriolar walls due to proliferation of smooth muscle cells. This process is best described by which of the following terms?
Which of the following is the characteristic histological feature of HIV-associated collapsing glomerulopathy?
Wilms tumor is associated with all of the following except?
A patient presents with one normal kidney and the contralateral kidney appearing contracted with evidence of scarring. What is the most probable diagnosis?
Most unlikely cause of acute tubular necrosis amongst the following is?
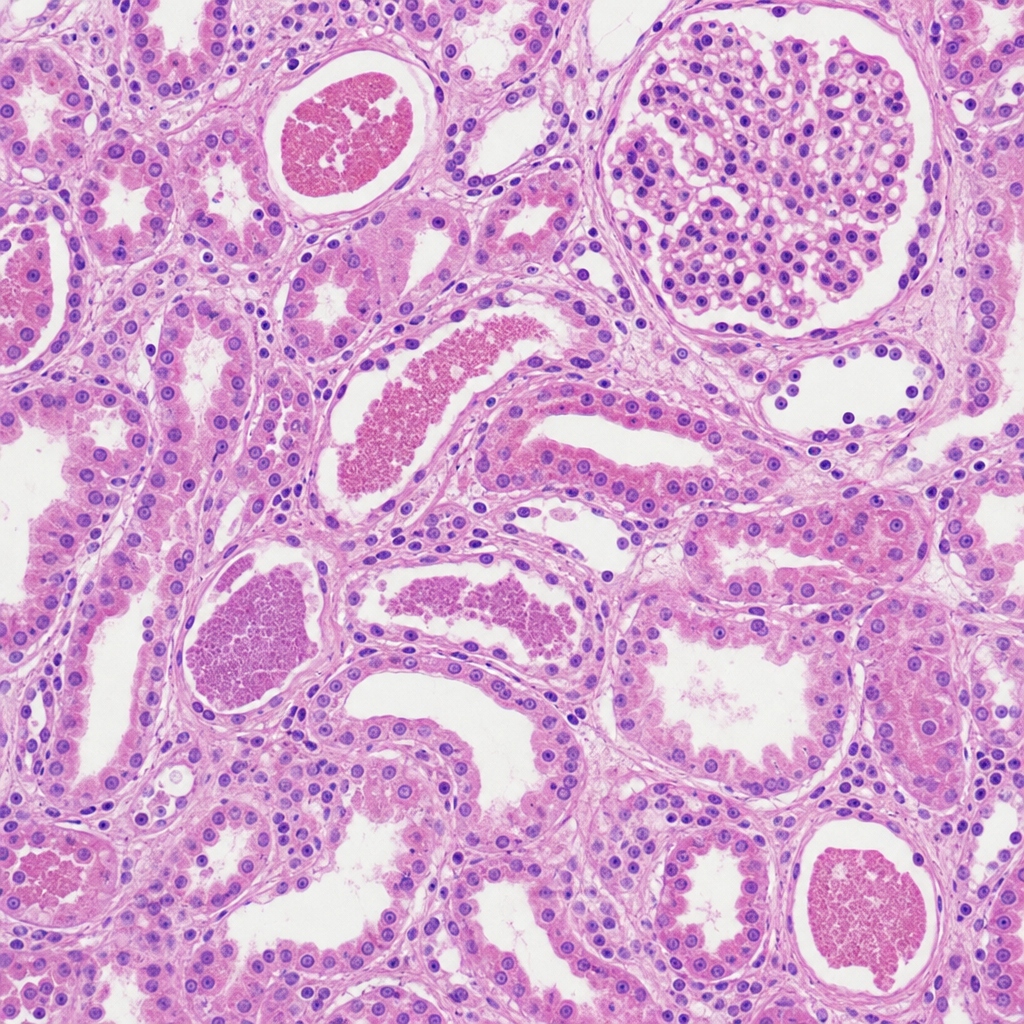
A 60-year-old man presents with acute renal insufficiency. He treated his garden last week with a number of herbicides and insecticides, some of which may have contained heavy metals. Laboratory studies confirm oliguria and increased levels of BUN (54 mg/dL) and creatinine (3.7 mg/dL). A renal biopsy is shown. What is the most likely diagnosis?
Dysmorphic RBCs with acute renal failure (ARF) are most commonly seen in which condition?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app