
Renal Pathology — MCQs

On this page
Crescents in renal pathology are derived from which of the following cellular components?
Malakoplakia of the bladder is associated with which of the following?
All are true about ANCA-associated crescentic glomerulonephritis, except?
What is the condition characterized by the triad of glomerulonephritis, pulmonary hemorrhages, and the presence of antibody to the basement membrane?
Presence of which of the following in the urine is diagnostic of glomerular injury?
What is the most common malignant tumor of the kidney in children?
Which type of Focal Segmental Glomerulosclerosis (FSGS) has the worst prognosis?
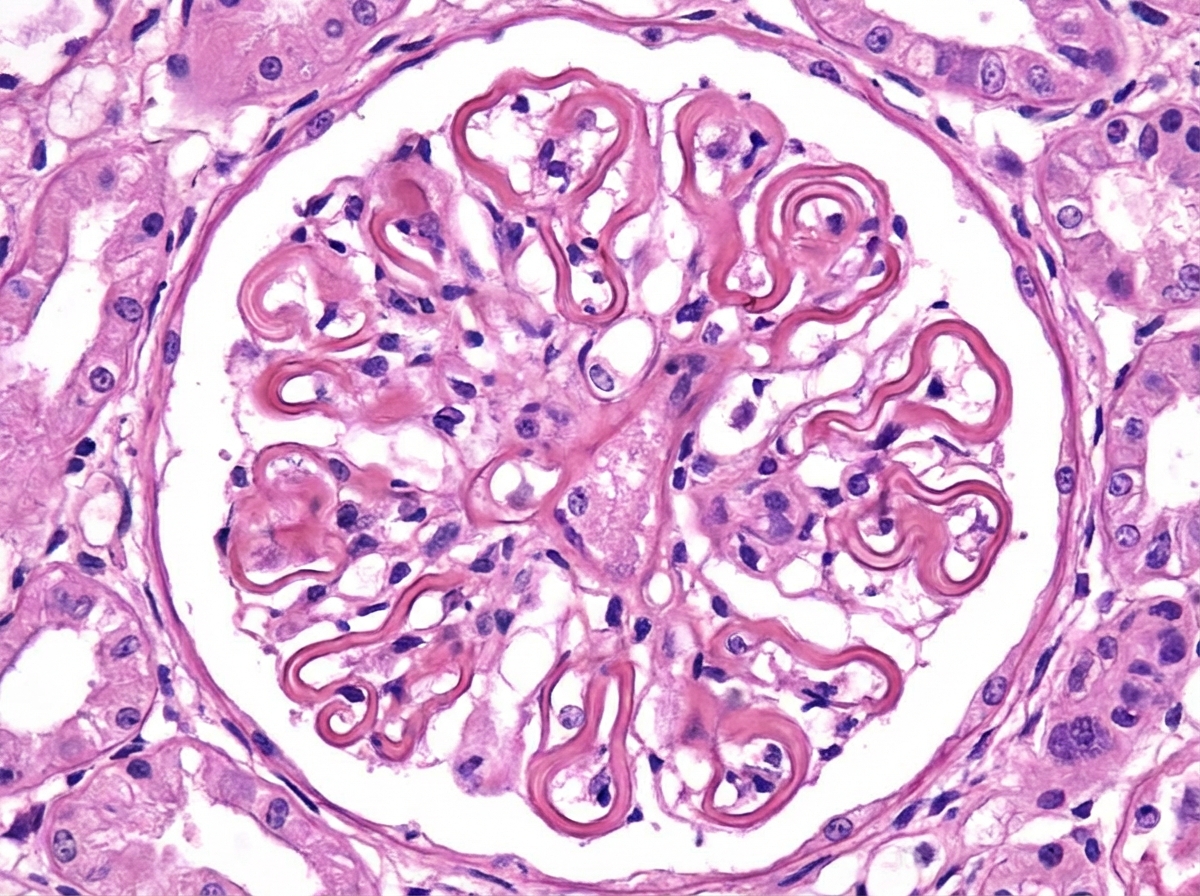
Which of the following diseases is characterized by the features presented?
A 45-year-old man has had poorly controlled hypertension for the past 11 years, with readings ranging from 150/90 mm Hg to 160/95 mm Hg. Over the last 3 months, his blood pressure has increased to 250/125 mm Hg. On physical examination, his temperature is 36.9°C, lungs are clear on auscultation, heart rate is regular, and there is no abdominal pain on palpation. A chest radiograph shows a prominent border on the left side of the heart. Laboratory studies show that his serum creatinine level has increased during this time from 1.7 mg/dL to 3.8 mg/dL. Which of the following vascular lesions is most likely to be found in this patient's kidneys?
In Wegener's granulomatosis, what are the characteristic histopathological features seen in the glomeruli?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app