
Renal Pathology — MCQs

On this page
If a kidney biopsy is done in a patient with bronchogenic carcinoma who presents with nephrotic syndrome, which lesion will most likely be seen?
A patient with chronic hypertension will show which of the following changes on histology of the kidney?
Which condition is characterized by wire loop lesions in the glomeruli?
The characteristic immunoglobulin abnormality in IgA nephropathy is:
Which of the following histological features is characteristic of Alport syndrome?
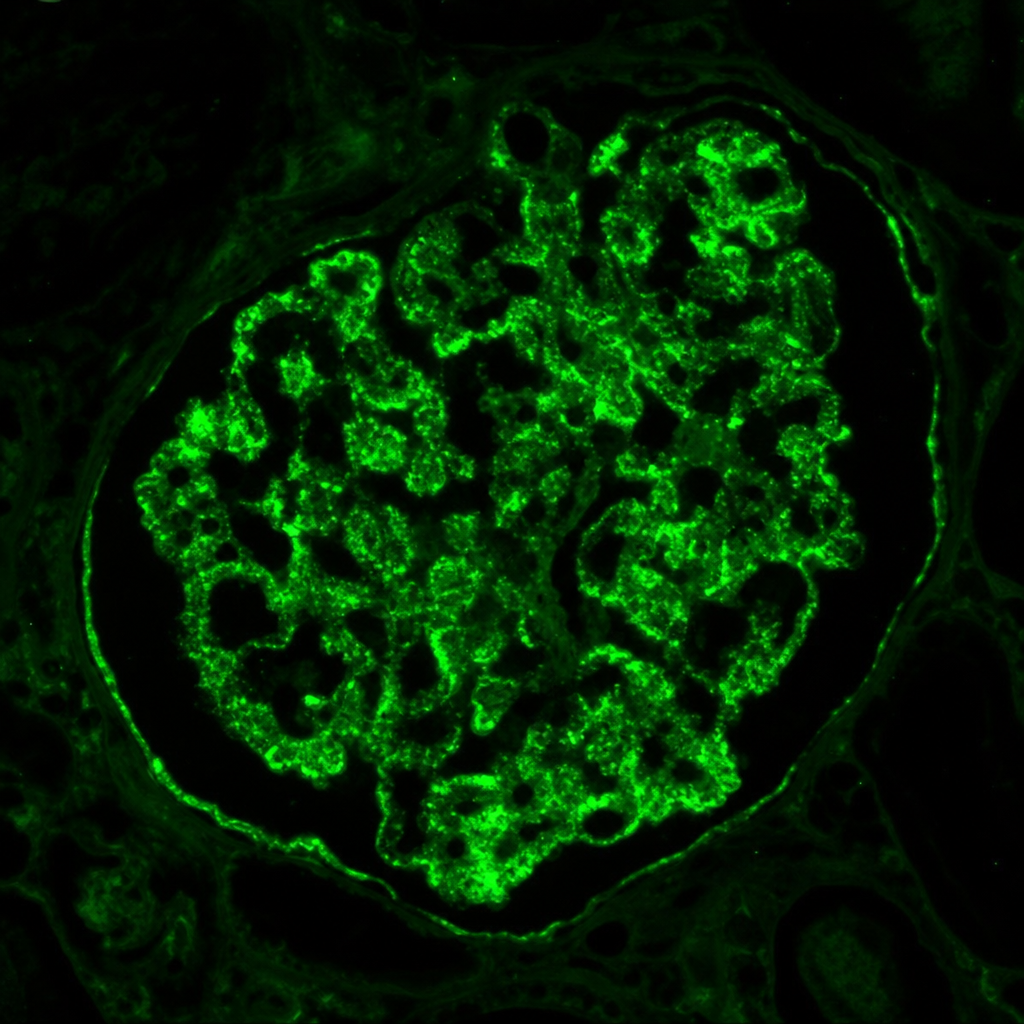
Immunofluorescence staining pattern from a kidney biopsy from a 35-year-old patient presenting with proteinuria, a malar rash, joint pain, and positive ANA and anti-dsDNA antibodies has been shown below. The immunofluorescence panel shows positivity for IgG, IgA, IgM, C3, and C1q (full-house pattern). What is the most likely diagnosis?
Michaelis-Gutmann bodies are seen in:
What is the mode of inheritance for the most common mutation in Alport syndrome, which is found in the COL4A5 gene?
A 40-year-old man presented with painless haematuria. Bimanual examination revealed a ballotable mass over the right flank. Subsequently, right nephrectomy was performed, and the mass was found to be composed of cells with clear cytoplasm. Areas of haemorrhage and necrosis were frequent. Cytogenetic analysis of this mass is likely to reveal the abnormality of which chromosome?
The cytogenetics of chromophilic renal cell carcinoma is characterized by:
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app