
Renal Pathology — MCQs

On this page
A 40-year-old woman with systemic lupus erythematosus (SLE) presents with symptoms including proteinuria, edema, and hypertension. What is the most likely renal pathology associated with her condition?
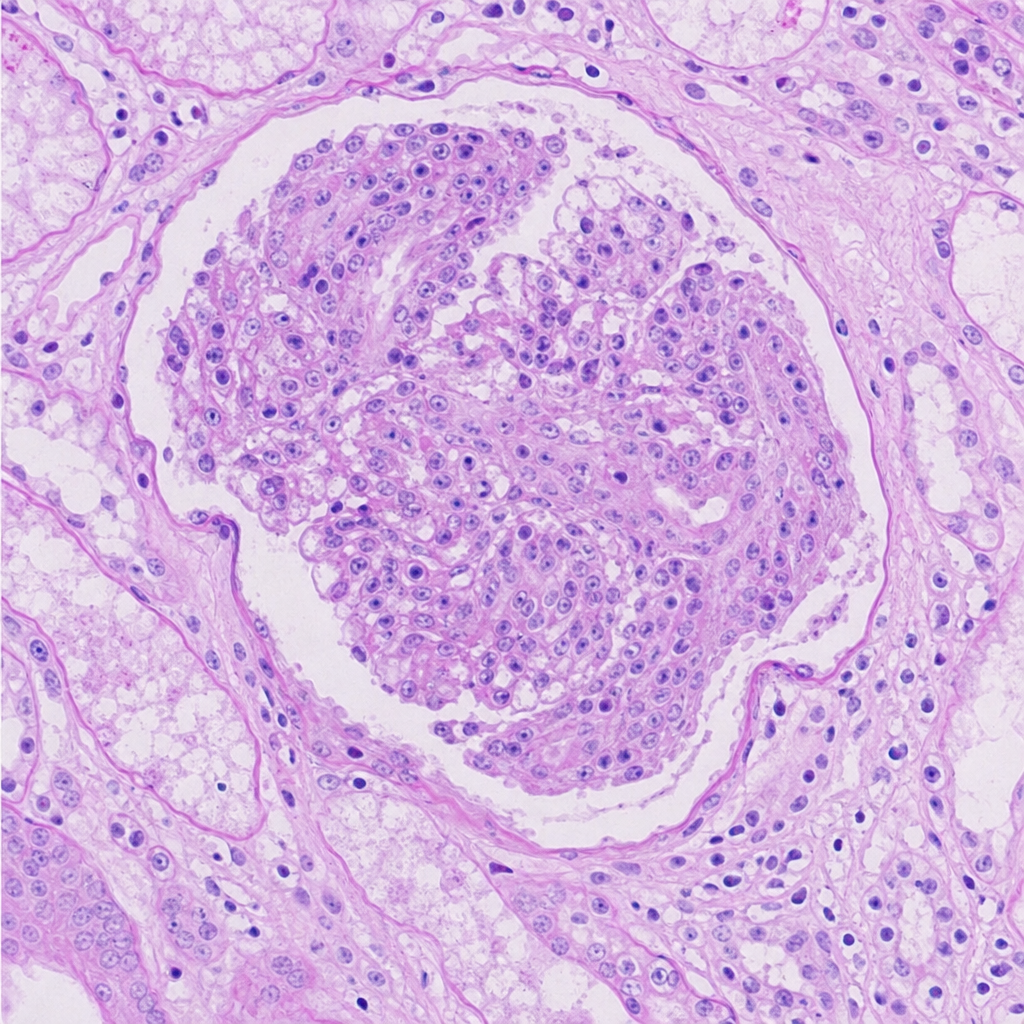
A 51-year-old person came with a complaint of hematuria. On examination, he was normotensive and had pedal edema. Investigations revealed the patient had no glucosuria and had a creatinine value of 9mg%. Renal biopsy is as shown below. Which of the following investigations should be done to identify the etiology of the disease?
Loss of foot process is classical in case of?
Struvite stones are primarily composed of which metal?
Which of the following is not a feature of Minimal change disease?
In a patient diagnosed with Autosomal Recessive Polycystic Kidney Disease (ARPKD), which protein is primarily altered due to mutations in the PKHD1 gene?
In a patient with nephrotic syndrome, which antibody is decreased?
Histopathology showing large cells with plant-like appearance and a perinuclear halo is seen in which type of renal cell carcinoma?
Which of the following statements about Renal Cell Carcinoma (RCC) is true?
Which of the following statements about Renal Cell Carcinoma (Hypernephroma) is true?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app