
Renal Pathology — MCQs

On this page
Autosomal dominant mutations in which one of the following genes may cause focal segmental glomerulosclerosis associated with abnormal genitalia, Wilms tumor and mental retardation?
All the following are features of Polycystic disease of kidneys EXCEPT:
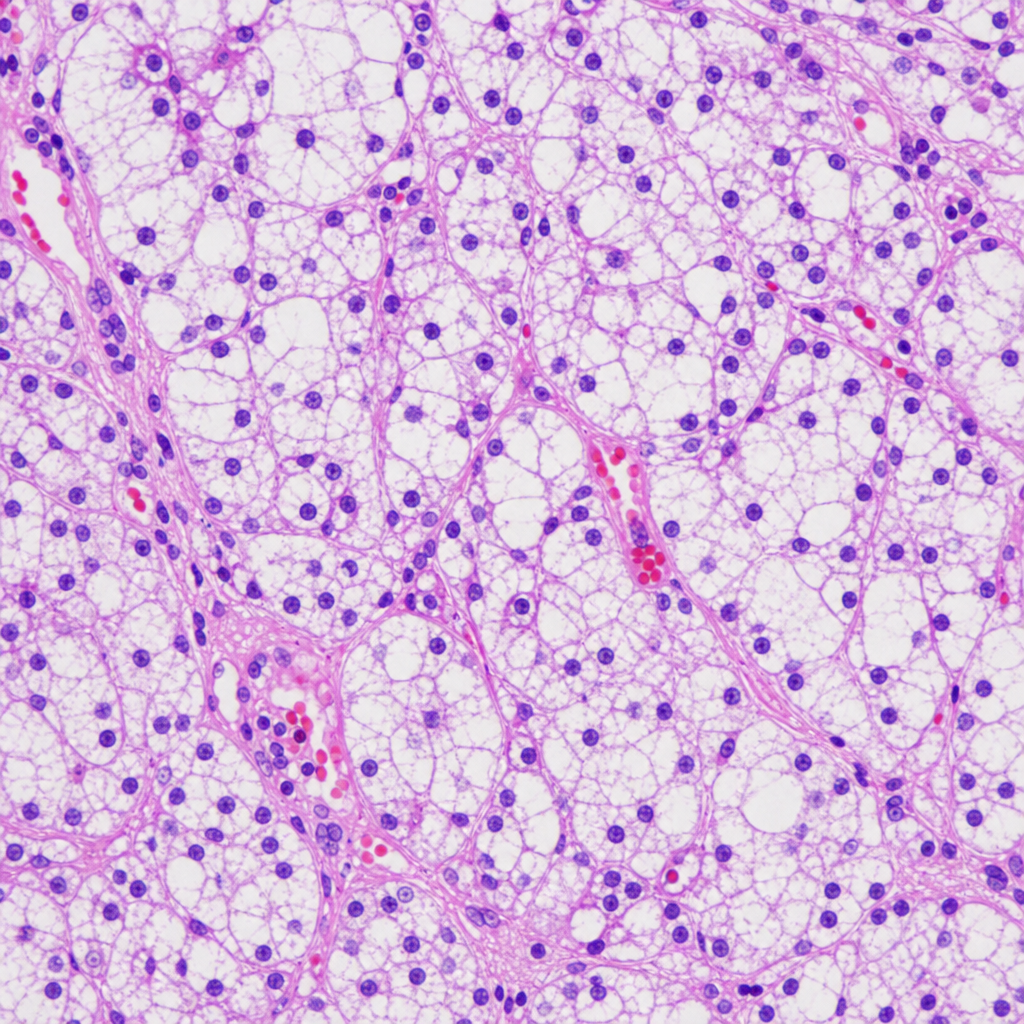
A patient presents with a renal mass leading to hematuria and flank pain. The histological image below is shown. What is the likely diagnosis? 
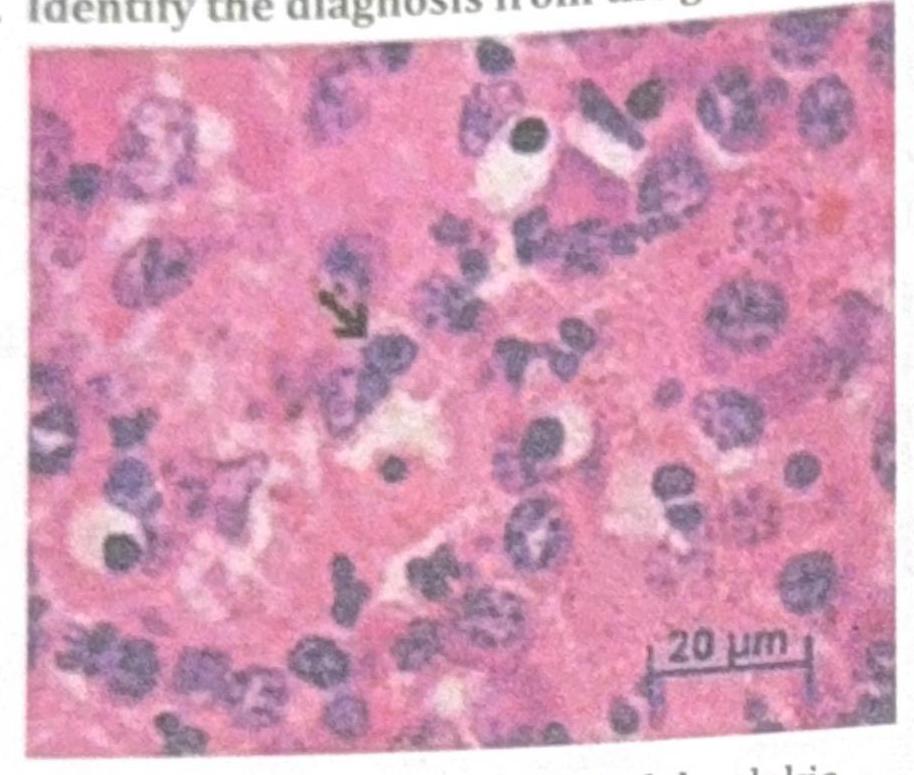
Identify the diagnosis from the given image
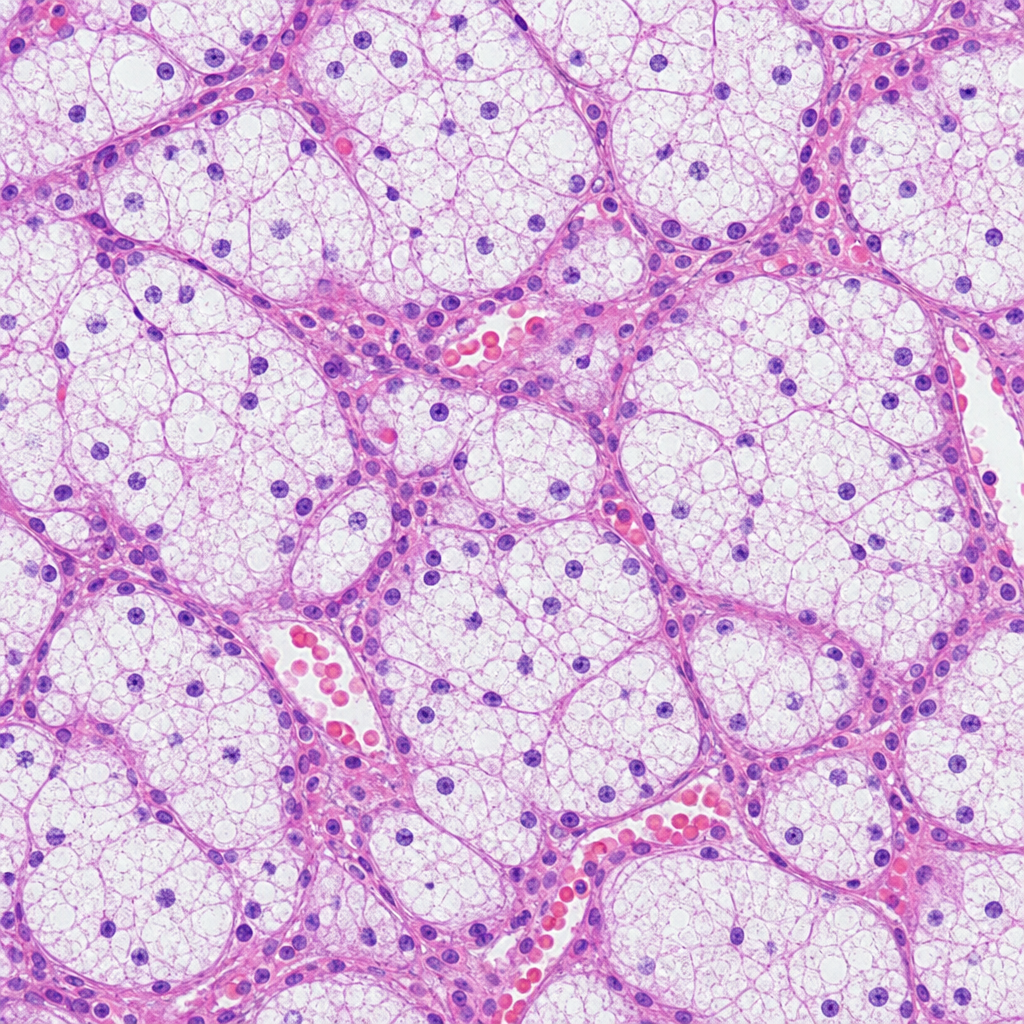
A patient presents with a renal mass leading to hematuria and flank pain. The histological image below is shown. What is the likely diagnosis?
A renal biopsy shows 'bamboo spine' pattern in arterioles. Which immunofluorescence finding would best support thrombotic microangiopathy?
A kidney biopsy shows 'tram-track' appearance on silver stain. Which immunofluorescence pattern would best support membranoproliferative glomerulonephritis?
A kidney biopsy under electron microscopy shows subepithelial 'spike' formation. Which immunofluorescence pattern would confirm membranous nephropathy?
In Goodpasture syndrome, which organ is involved apart from the lung?
Crescent forming glomerulonephritis is:-
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app