
Renal Pathology — MCQs

On this page
A patient with renal disease undergoes a biopsy. On Congo red staining, the deposits show apple-green birefringence under polarised light. What is the most likely diagnosis?
A 5-year-old child presented with a history of edema of the face which later progressed to generalized edema. Urine showed massive proteinuria and light microscopy was normal. Electron microscopy showed effacement of podocyte foot processes. What is the diagnosis?
Tamm-Horsfall mucoprotein is a major component of which of the following?
Least common finding in diabetic kidney is
In renal transplant biopsy, which of the following stains is not used to identify organisms?
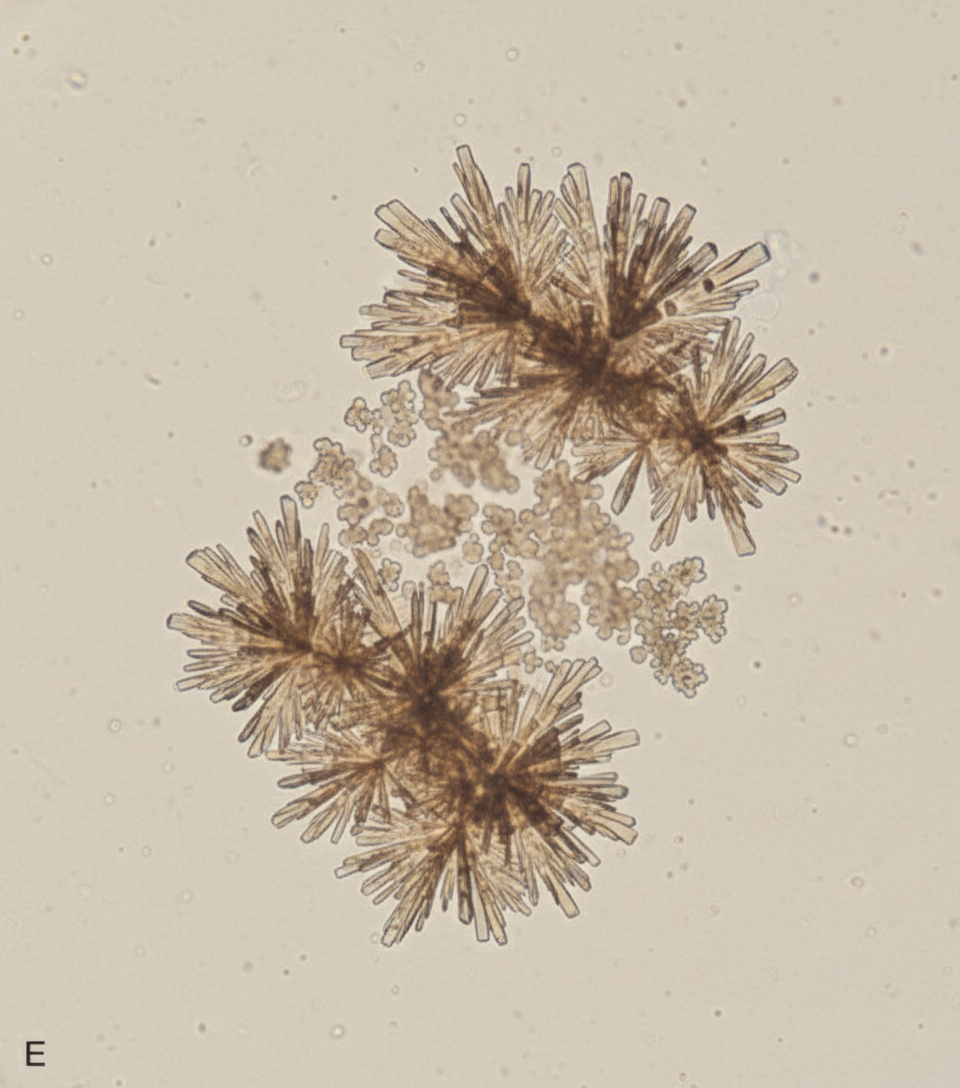
A 6-year-old child presents with recurrent urinary tract infections. Urine microscopy findings are shown in the image below. What type of crystalluria is depicted?
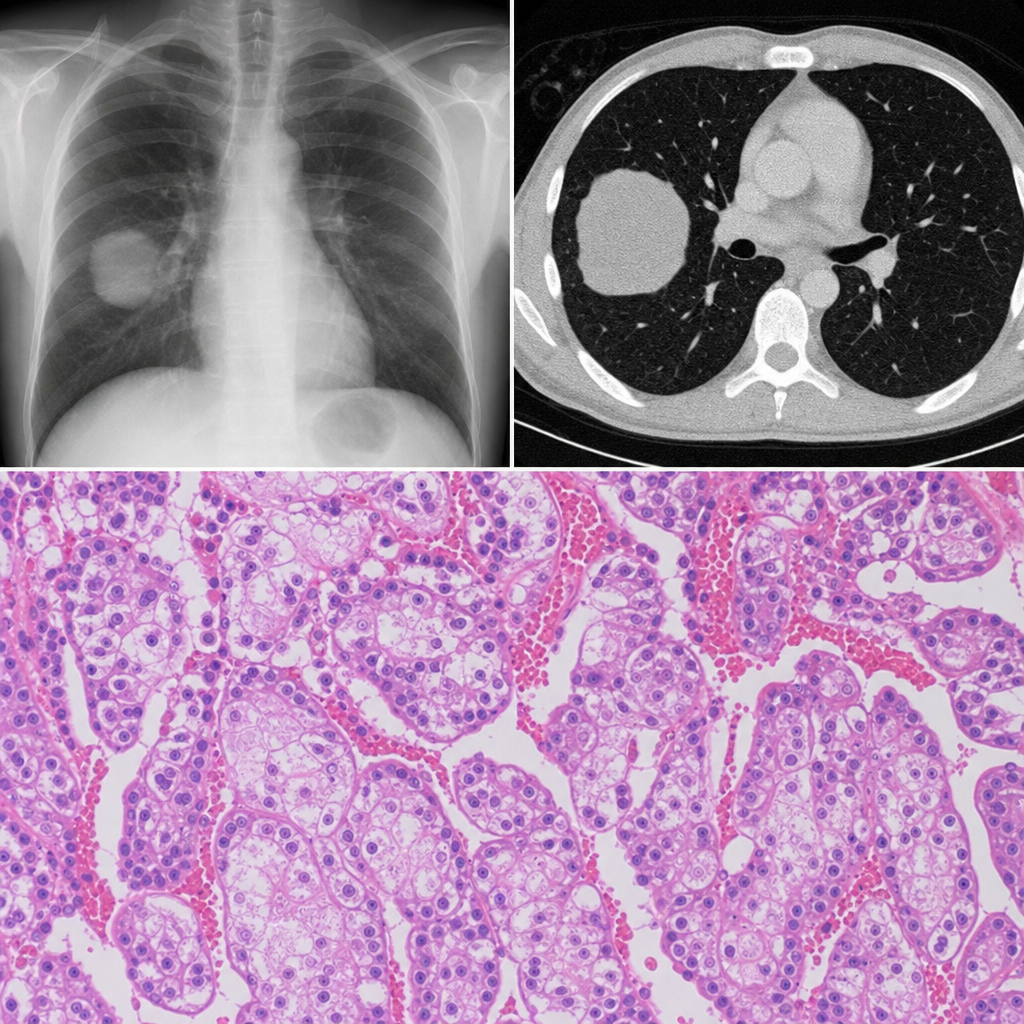
On the basis of radiopathological correlation. What is the diagnosis?
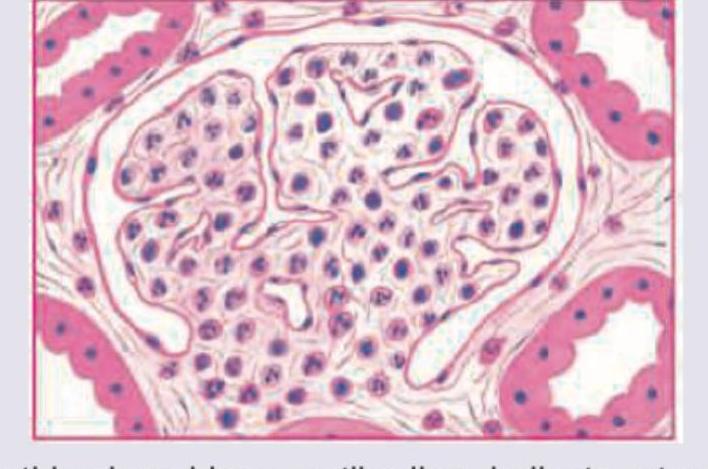
A 6-year-old child presents with puffy eyes, scanty urination. On examination BP=130/80 mmHg and urine examination shows RBC casts. Kidney biopsy specimen is given below. Which of the following is incorrect about the diagnosis of this child?
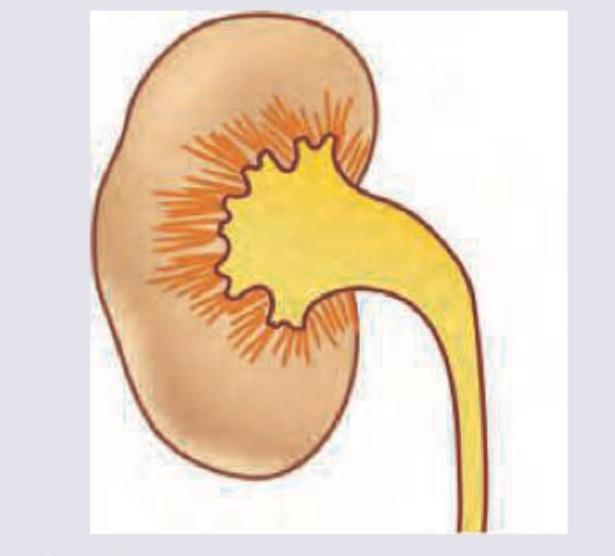
What is the most common extra-renal manifestation in this condition showing small cysts radiating peripherally from the medulla?
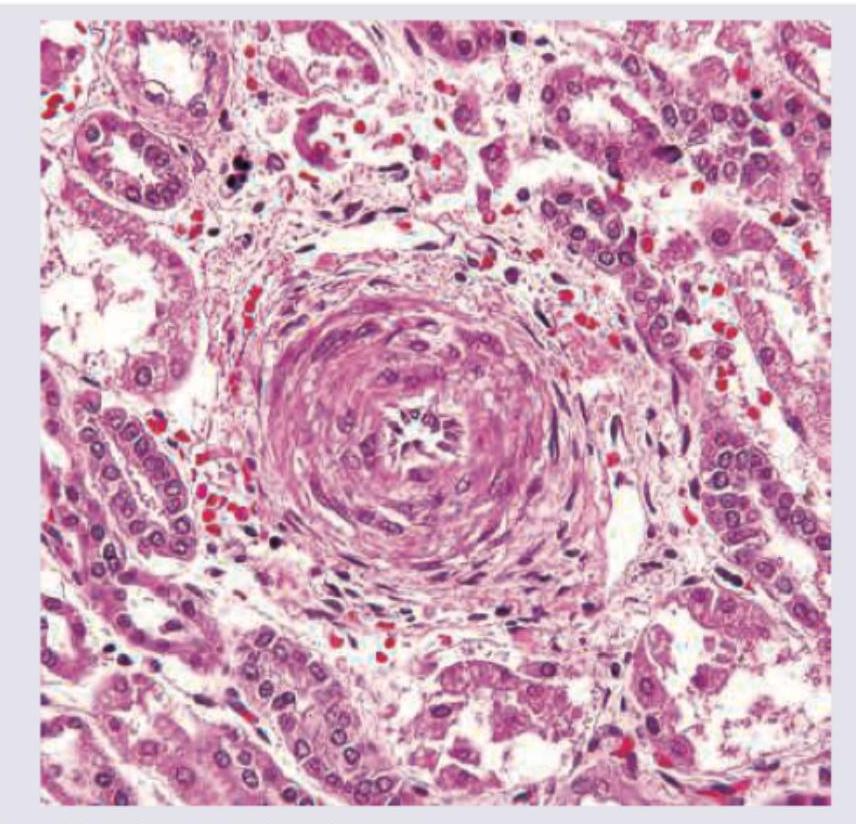
A 45-year-old male with severe hypertension presents with acute renal failure. A renal biopsy shows the histopathological findings in the image. What is the most likely diagnosis?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app