
Renal Pathology — MCQs

On this page
Transitional cell carcinoma of the bladder is associated with which of the following?
Glomerulonephritis is due to what mechanism?
Hyaline casts are seen in which of the following conditions?
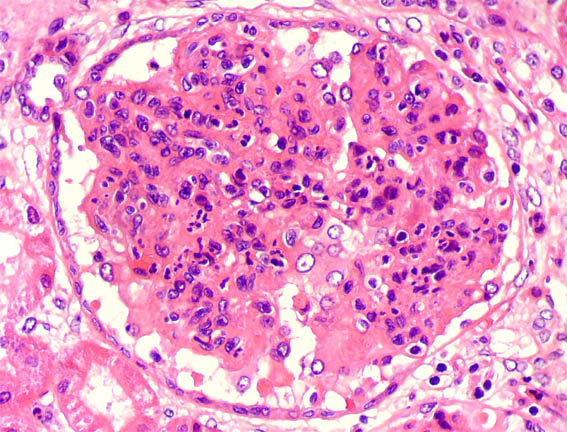
A 8-year-old boy presents 2 weeks after a sore throat with hematuria, periorbital edema, and hypertension. Serum C3 is low and ASO titer is elevated. Examine the renal histopathology slide. What is the probable diagnosis?
The gross specimen shows a Mallory-Weiss tear at the gastroesophageal junction. The disease process that best accounts for this problem?

Hobnail pattern is seen in which type of Renal Cell Carcinoma?
Type I RPGN is seen in which of the following conditions?
Which chromosome is involved in Wilm's tumor?
Which of the following is a feature of autosomal recessive polycystic kidney disease?
Chronic urethral obstruction due to benign prostatic hyperplasia can lead to which change in the kidney parenchyma?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app