
Renal Pathology — MCQs

On this page
In thin basement membrane disease, the defect is in which component?
Familial Renal Cell Carcinoma is associated with which of the following genetic syndromes?
What is the most common renal pathology observed in patients experiencing shock?
Goodpasture's disease is characterized by all of the following except:
Which of the following conditions is characterized by occasional breaks in the glomerular basement membrane and subepithelial deposits visible on electron microscopy?
Which of the following features characterize Hemolytic Uremic Syndrome?
What is true about acute post-infective glomerulonephritis?
At autopsy, a patient who had died with acute anuria and uremia is found to have ischemic necrosis of the cortex of both kidneys with relative sparing of the medulla. These pathological findings are MOST likely related to which of the following underlying conditions?
Wire loop lesions are often characteristic for which class of lupus nephritis?
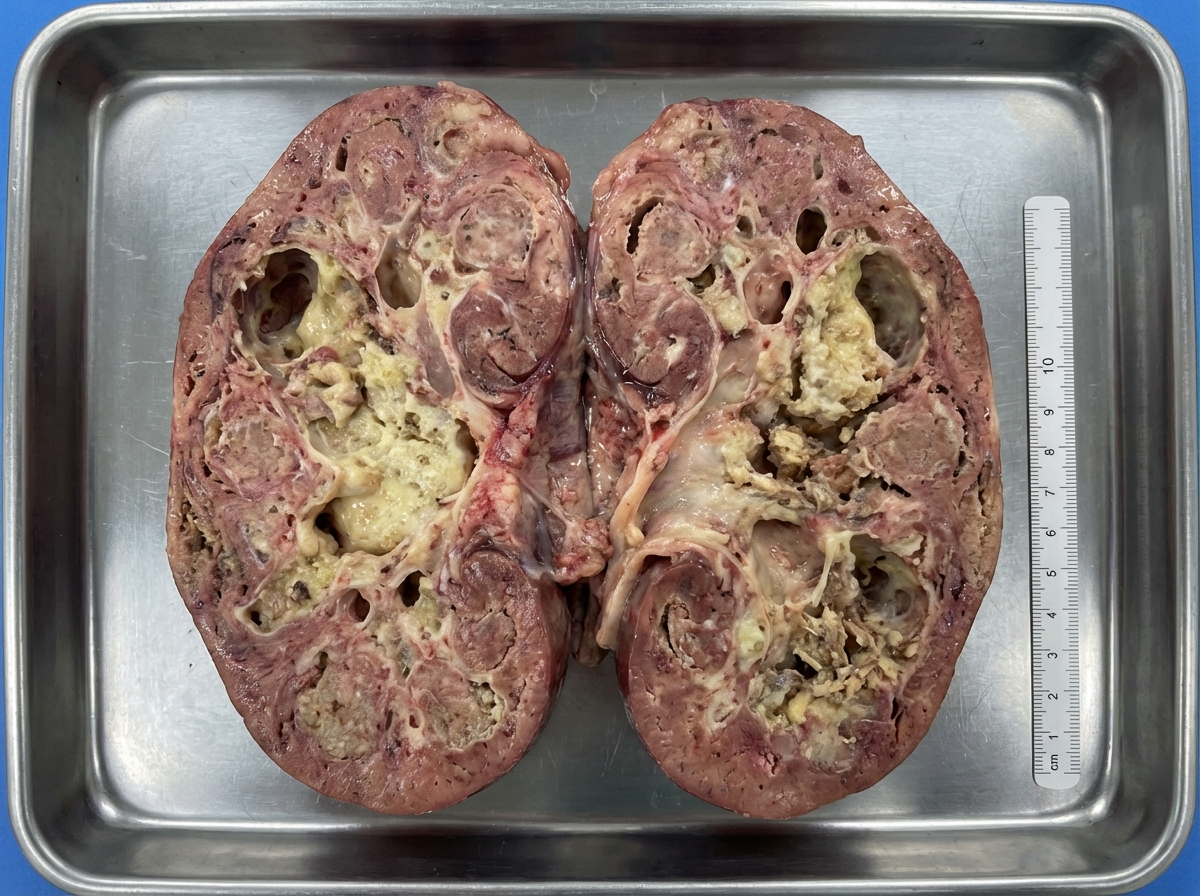
A patient presented with pus in urine. Urine culture was negative. Following a sudden onset of renal failure, the patient died. An autopsy revealed the following finding in the kidney. What is the most likely diagnosis?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app