
Renal Pathology — MCQs

On this page
In Paneth cells, cysts are seen in all of the following locations except?
Which of the following is NOT a typical electron microscopic feature of Alport syndrome?
Which of the following is a characteristic histological finding in Alport syndrome?
The important light microscopical features in Alport syndrome are all, EXCEPT:
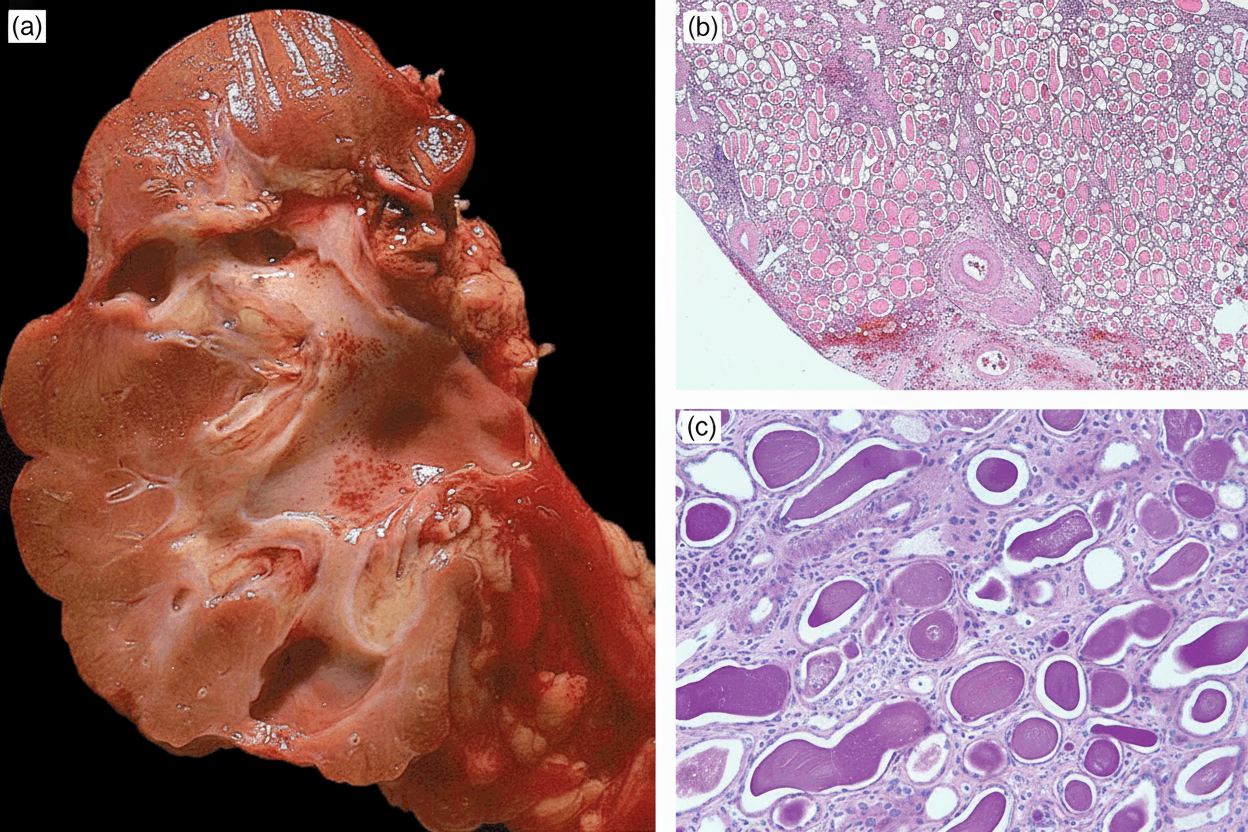
A 45-year-old male with a history of recurrent ureteric calculi presented with fever. Following right-sided nephrectomy, gross and histological views were obtained. What is your diagnosis?
If urine dipstick shows +3 for protein, what is the approximate protein level in mg/dl?
SUPAR is a blood marker for which of the following conditions?
Which one of the following is not a feature of clear cell carcinoma of the kidney?
An IV drug abuser develops an aggressive form of nephrotic syndrome that does not respond to steroids. A renal biopsy is performed. Which of the following histological diagnoses will most likely be made from the biopsy tissue?
A 14-year-old girl presents with a 5-day history of hypertension, oliguria, and hematuria. She was seen 2 weeks earlier for a severe throat infection with group A beta-hemolytic streptococci. A kidney biopsy displays glomerulonephritis. Immunofluorescence staining for which of the following proteins would provide the strongest evidence that this patient's glomerulonephritis is mediated by immune complexes?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app