
Renal Pathology — MCQs

On this page
What is the most common tumor of the urinary bladder?
Which of the following is NOT a pathological change seen in diabetic nephropathy?
Renal pathology in SLE includes all EXCEPT?
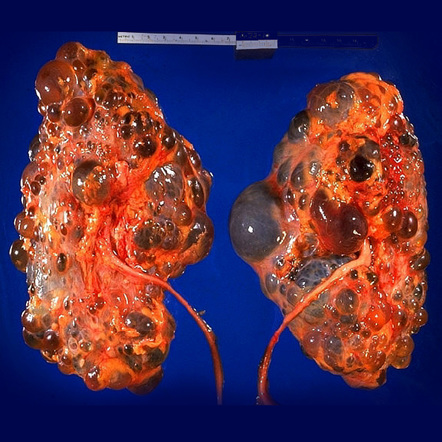
Distal and collecting duct cysts are seen in which condition?
Which of the following is NOT true about the condition shown?
Pulsatile metastases are seen in which cancer?
What is the characteristic pathological finding in the kidney in malignant hypertension?
A child presents with an abdominal mass. Biopsy showed a triphasic tumor. Which of the following is a characteristic feature of this tumor?
According to WHO, which feature characterizes Class II lupus nephritis?
The characteristic feature of benign nephrosclerosis is
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app