
Renal Pathology — MCQs

On this page
A 37-year-old man develops pulmonary hemorrhage and glomerulonephritis. Lung biopsy with immunofluorescence demonstrates IgG deposition along the basement membrane. These antibodies are most likely directed against which of the following types of collagen?
What are the histological features of acute rejection of a renal transplant?
Which of the following conditions is characterized by highly selective proteinuria?
Immune complex-mediated glomerular damage is seen in all except?
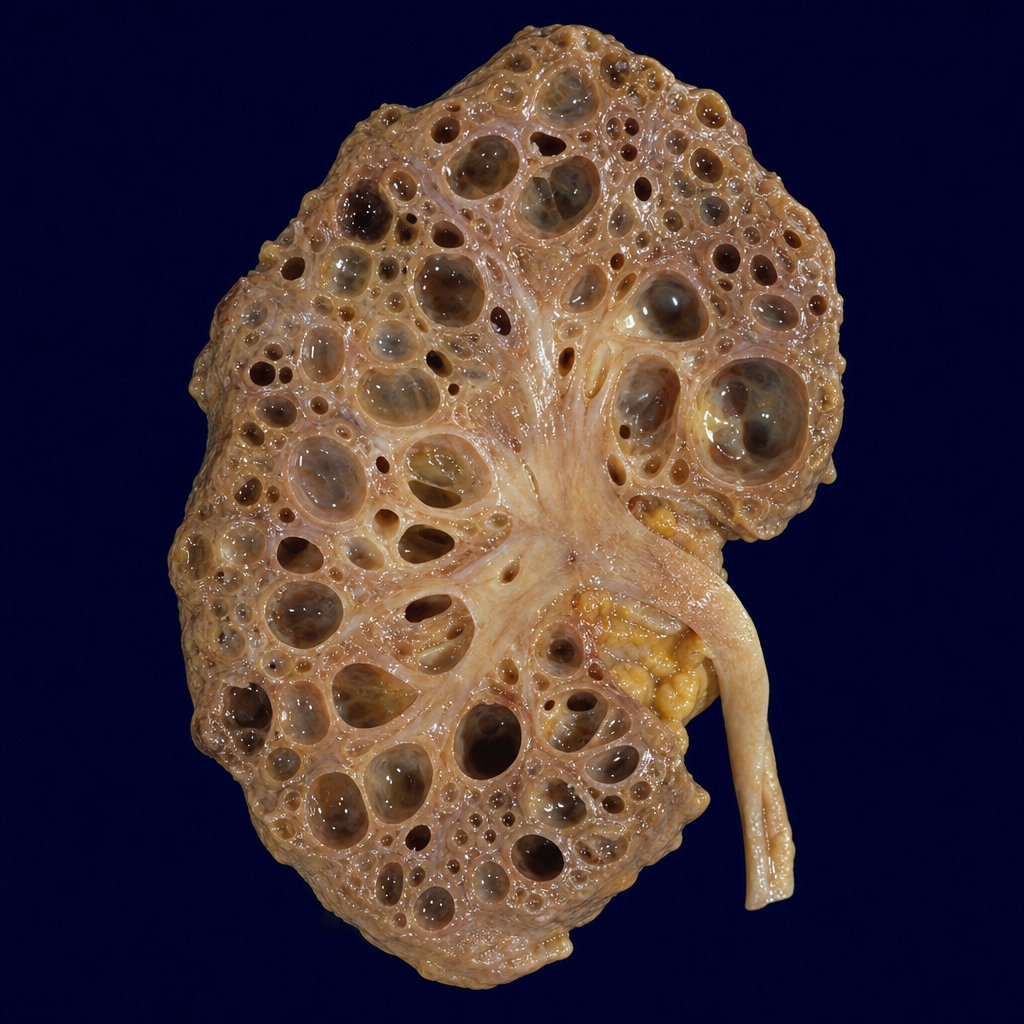
The gross specimen section of kidney depicts which of the following?
Complement level is reduced in which of the following conditions?
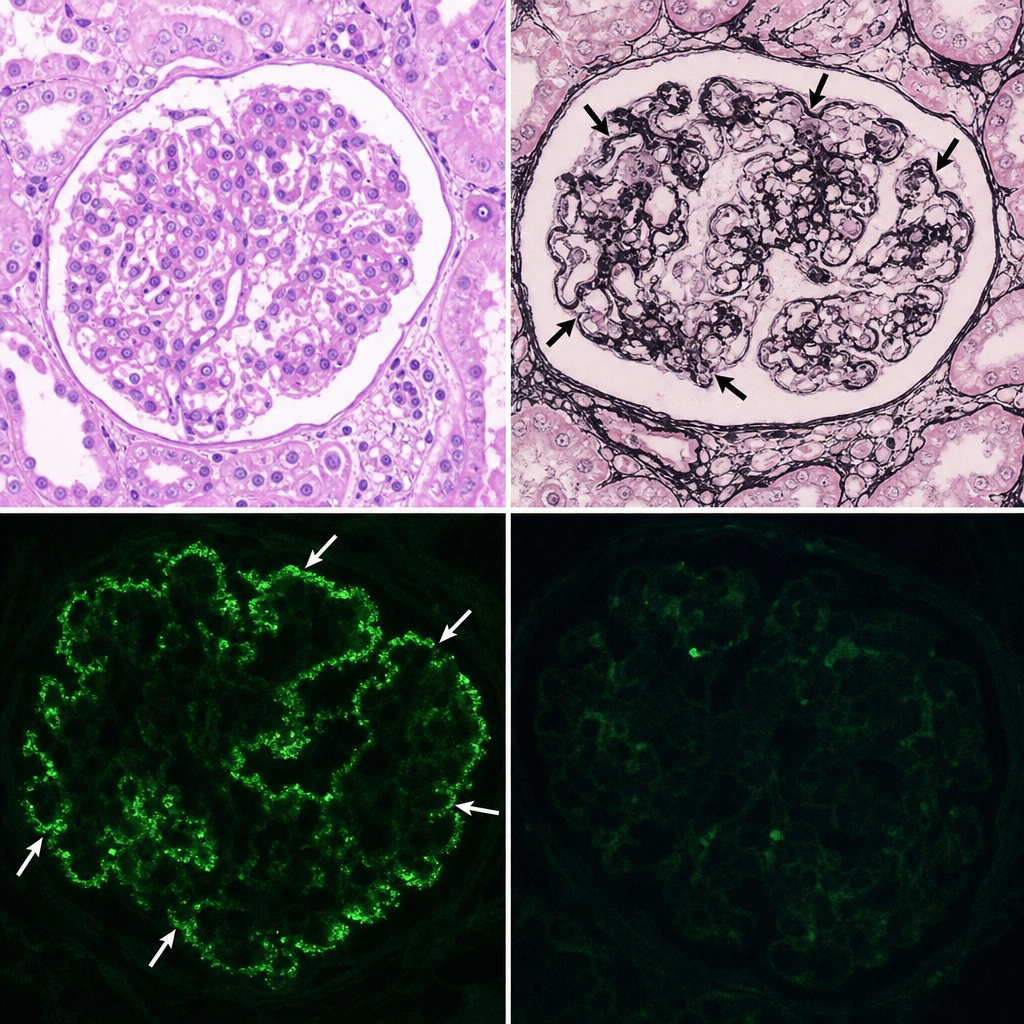
A 75-year-old female patient presented with microscopic hematuria with RBC casts seen in the urine. Her serum creatinine was 3.9 mg/dl. Light microscopy and silver staining of the kidney specimen revealed specific findings. Which of the following would be the most appropriate diagnosis and the site of Ig deposits?
What is the commonest cause of renal papillary necrosis?
What is the most common cause of glomerulonephritis?
What is the most common type of urinary stone associated with urinary tract infections?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app