
Renal Pathology — MCQs

On this page
Cholemic nephrosis is seen in:
Which of the following is a cause of leprosy?
KIM-1 is a novel biomarker for which of the following conditions?
Renal calculi associated with Proteus infection are typically composed of which substance?
Which of the following conditions is associated with pauci-immune crescentic glomerulonephritis?
A patient presented with hematuria and acute renal failure. Renal biopsy showed crescentic glomerulonephritis with immunofluorescence findings of C3 and IgG deposition. What is the most likely diagnosis?
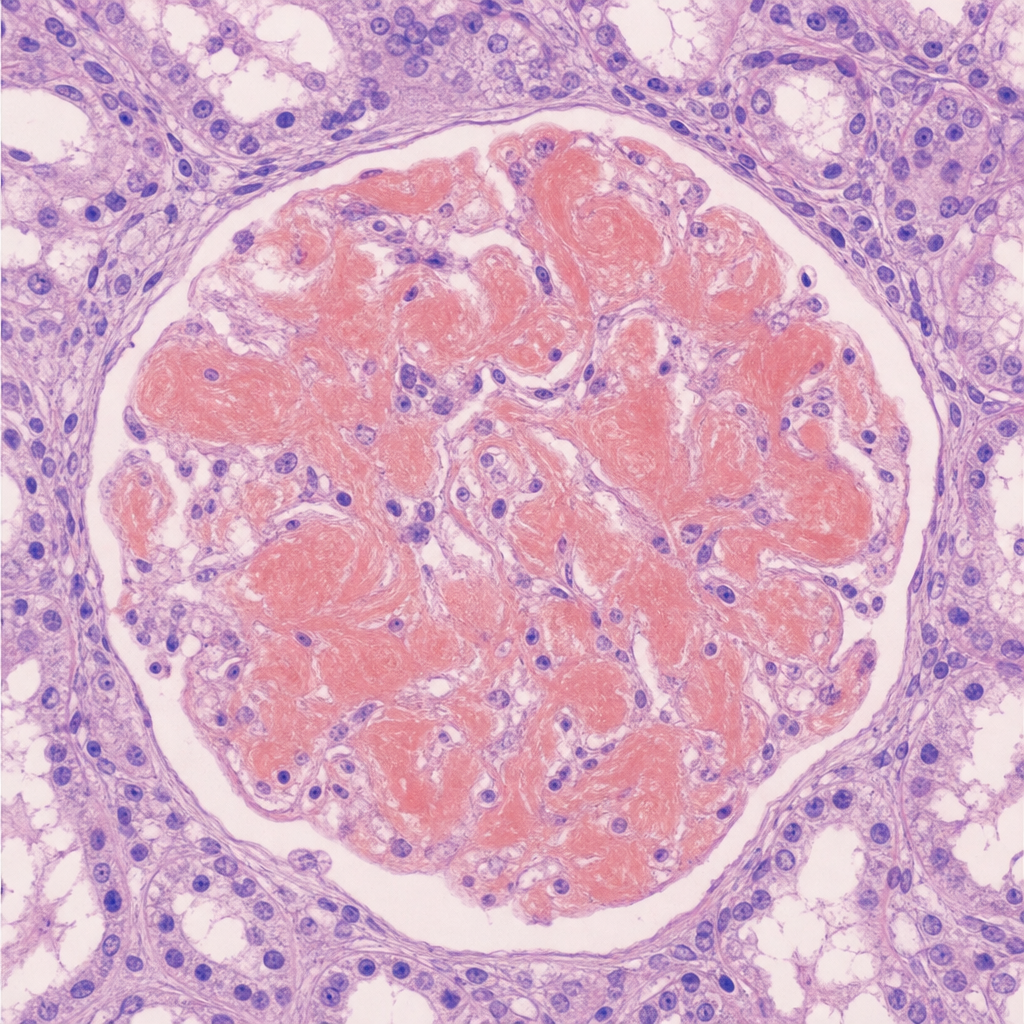
Renal biopsy findings are shown in this image. What is the most probable diagnosis?
In the rejection phenomenon after kidney transplant, what is the primary target for early immunological attack?
Which of the following statements about Renal Cell Carcinoma (Hypernephroma) is false?
Which of the following is a feature of septic shock?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app