
Renal Pathology — MCQs

On this page
What is the first manifestation of Alport syndrome?
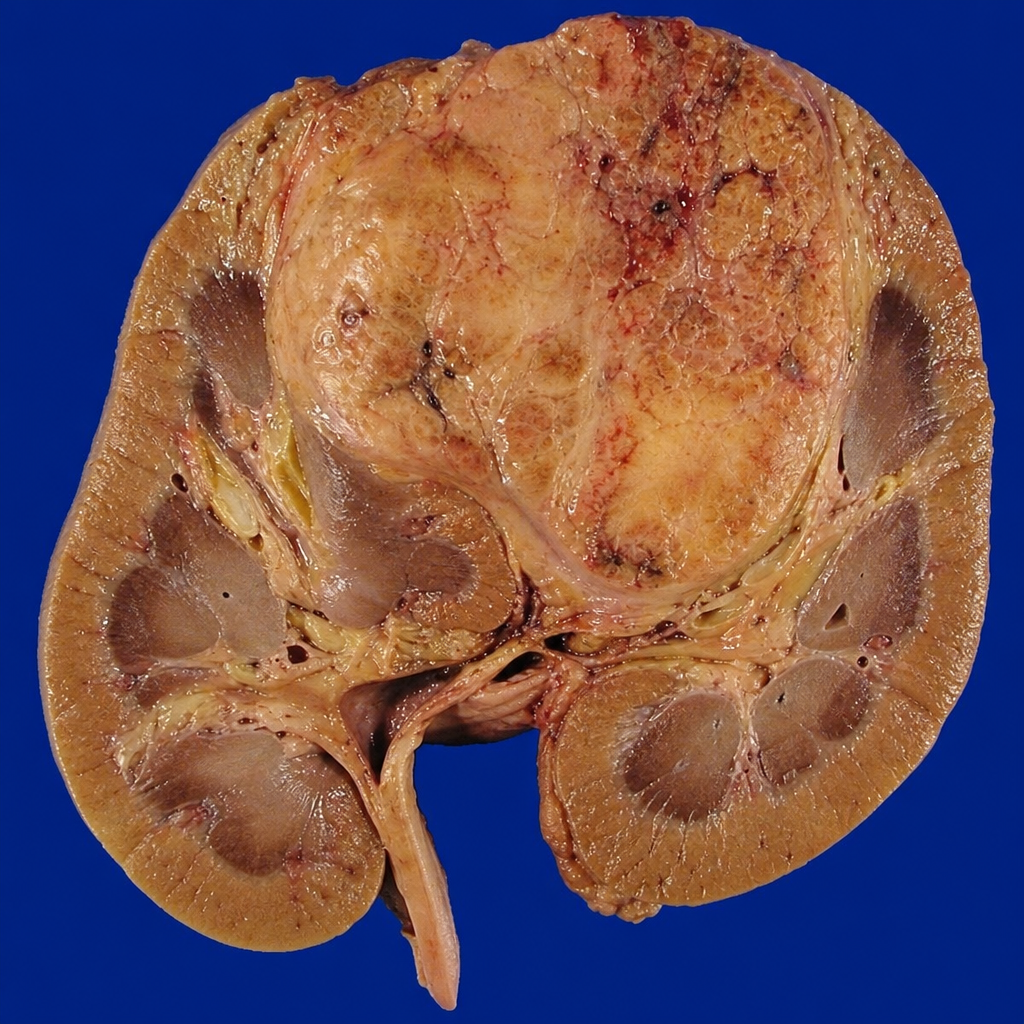
A specimen shows a nephrectomy. What is your diagnosis?
Which is the most characteristic glomerular nephritis (GN) in HIV patients?
What is the most common renal tumour?
Bilateral renal cell carcinoma is seen in which of the following conditions?
All of the following are causes of acute tubular necrosis (ATN) except?
Flea bitten kidney is seen in all of the following conditions except?
All of the following are causes of granular contracted kidney except?
All of the following are true about thin basement membrane defect, except:
Which chromosomes are involved in adult polycystic kidney disease (APKD)?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app