
Renal Pathology — MCQs

On this page
A 20-year-old primigravid woman in her third trimester reports minimal fetal movement. Ultrasound reveals bilaterally enlarged echogenic kidneys and a markedly decreased amniotic fluid index. The patient delivers a stillborn male fetus at 33 weeks' gestation. Autopsy shows deformations consistent with marked oligohydramnios, including flattened facies, varus deformities of the feet, and severe pulmonary hypoplasia. Microscopic examination of the liver reveals multiple epithelium-lined cysts and bile duct proliferation. What is the most likely renal disease in this fetus?
A person with radiologically confirmed reflux nephropathy develops nephrotic range proteinuria. Which of the following would be the most likely histological finding in this patient?
Rapidly progressive glomerulonephritis is characterized by which of the following?
All of the following conditions can cause interstitial nephritis except?
Which of the following markers is NOT characteristically positive in Wilms tumor?
What is the most common pathological feature in diabetes mellitus?
Azotemia occurs when:
A 50-year-old male presented with blurring of vision. Urine examination showed proteinuria. Fundus examination showed dot-and-blot hemorrhages, microaneurysms, and cotton wool spots. What is the most probable diagnosis based on the provided histopathology?
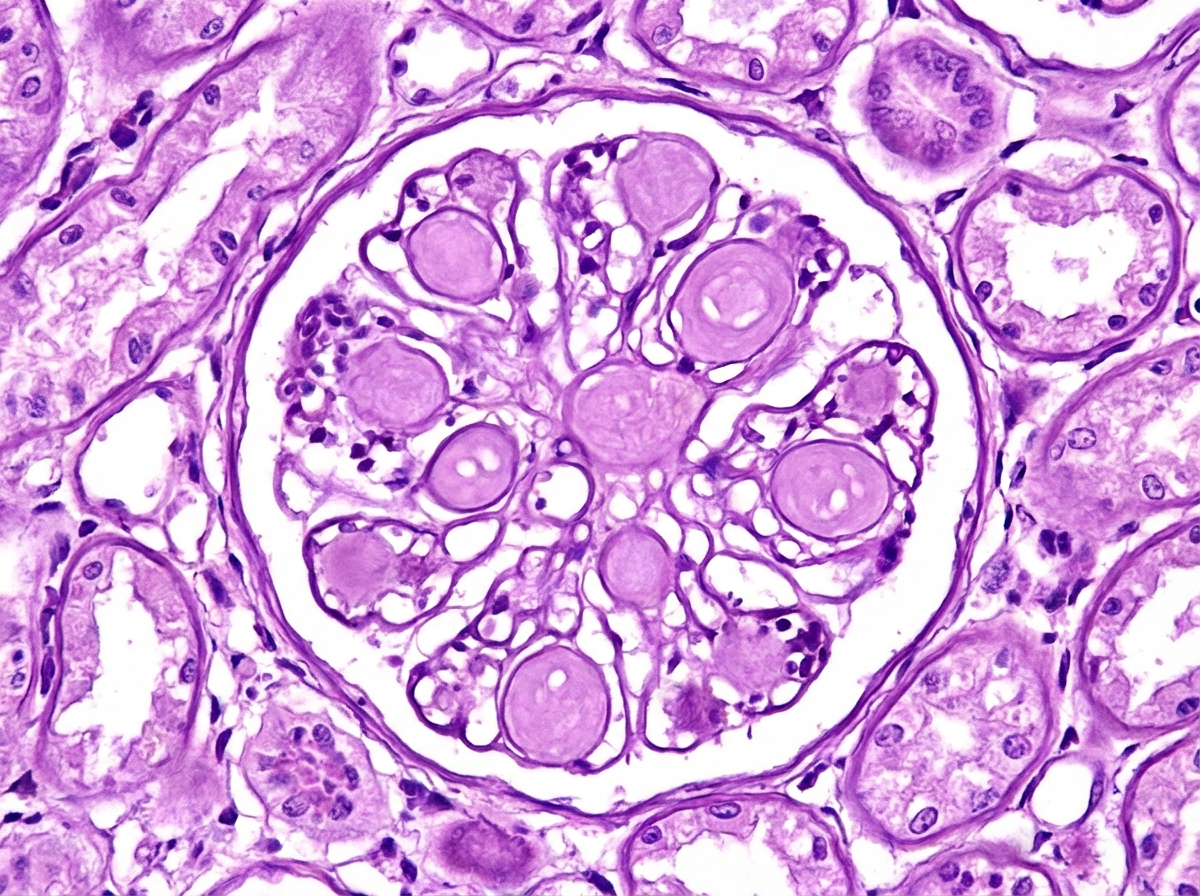
An elderly male patient presented with blurring of vision. Fundus examination revealed cotton wool spots on retina and systemic examination showed decreased peripheral sensations and increased urine output. What finding is shown on renal biopsy?
Renal pathology in SLE includes all EXCEPT?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app