
Renal Pathology — MCQs

On this page
What is the most common cause of glomerulonephritis?
IgA nephropathy is characterized by which of the following glomerular changes?
Which of the following is rarely associated with renal cell carcinoma?
Which condition is characterized by the presence of WBC casts?
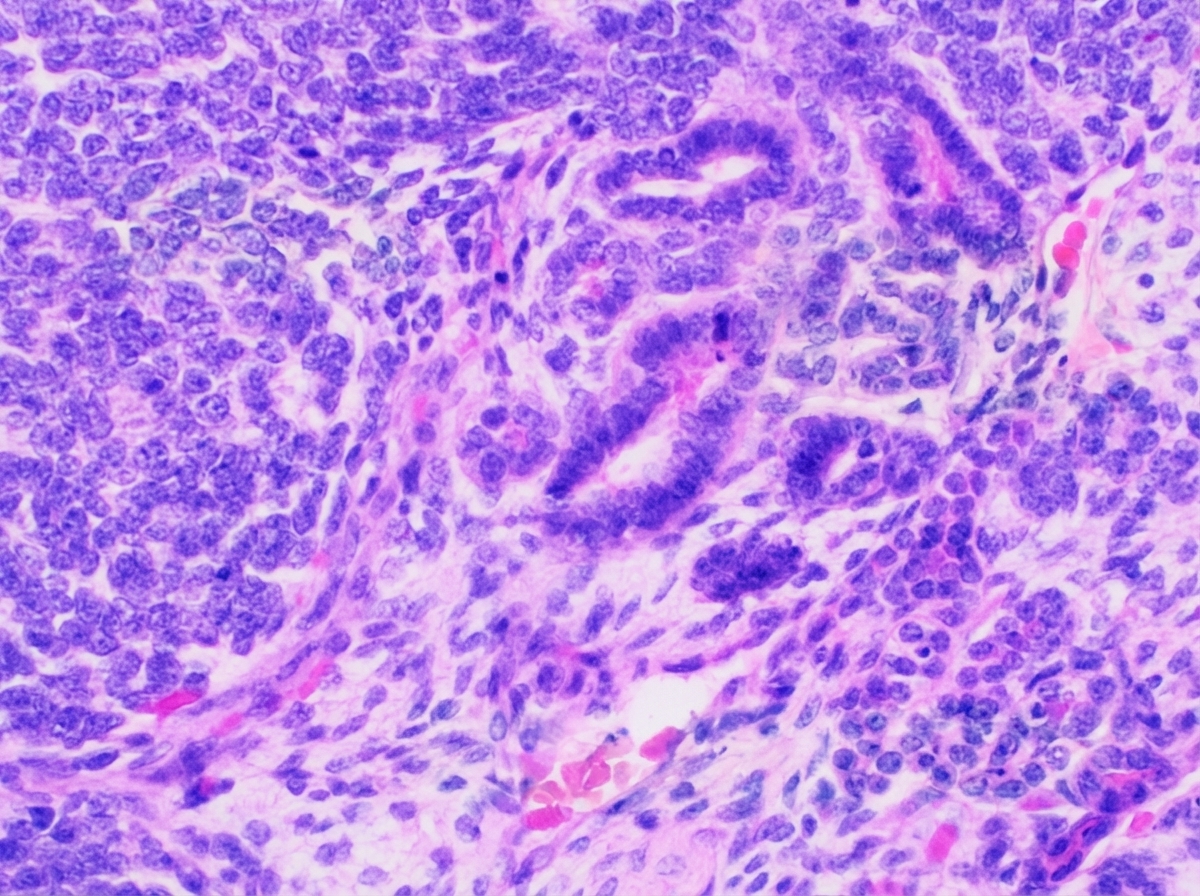
A 4-year-old child presented with a palpable abdominal mass in the right flank region which was painless and slowly increasing in size along with some episodes of fever and hematuria. On examination, hypertension was noted. CT scan of the abdomen was done. The patient was operated and the mass was resected. The histopathology image is given below. All of the following genes can be mutated in the above disease except?
A middle-aged diabetic female presented with flank pain and fever. On ultrasound, the kidney was irregular and showed a fat-density lesion with calculi. What is the most probable diagnosis?
Which of the following statements is true regarding kidney tumors?
A 65-year-old man develops oliguria and peripheral edema over a period of weeks. Urinalysis reveals hematuria and proteinuria; examination of the urinary sediment reveals red cell casts. Radiological and ultrasound studies fail to demonstrate an obstructive lesion. Renal biopsy shows many glomerular crescents. This presentation is most suggestive of which of the following conditions?
Which of the following conditions is associated with pauci-immune crescentic glomerulonephritis?
What is the most common variant of renal cell carcinoma (RCC)?
Practice by Chapter
Congenital Anomalies of the Kidney
Practice Questions
Glomerular Diseases
Practice Questions
Tubular and Interstitial Diseases
Practice Questions
Vascular Diseases of the Kidney
Practice Questions
Cystic Diseases of the Kidney
Practice Questions
Urinary Tract Obstruction and Stones
Practice Questions
Renal Tumors
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Renal Transplantation Pathology
Practice Questions
Urinary Tract Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app