
Neuropathology — MCQs

On this page
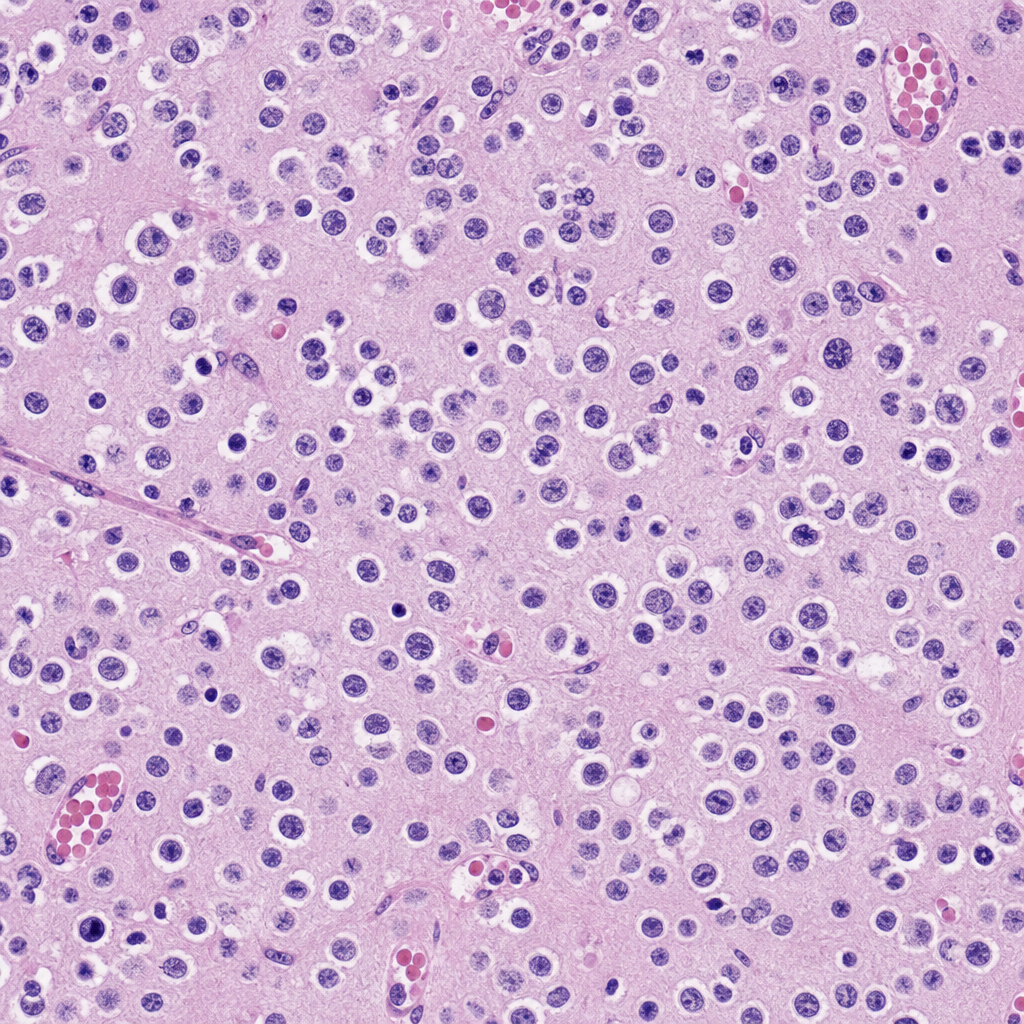
A 45-year-old patient presented with neurological deficits and seizures. Imaging showed a lesion in the temporal lobe. Biopsy of the lesion was taken for histological examination. Based on the characteristic histological features, what is the most likely diagnosis?
Neurofibrillary tangles are a deposition of which of the following substances?
Neurodegeneration with iron accumulation in basal ganglia is typically seen in which condition?
What is the most common primary brain tumor in adults?
Rupture of Berry aneurysm causes which type of hemorrhage?
Small cystic lesions in the lenticular nucleus, thalamus, and internal capsule are most closely associated with what condition?
Which of the following statements is FALSE regarding Krabbe's disease?
What is the most common type of pathological change seen in Rabies?
What is a watershed infarct in the brain?
A 12-year-old boy develops fever, accompanied by occasional headaches, malaise, fatigue, and nausea a month after being bitten by a dog. One day later, he experiences episodes of rigidity, hallucinations, breath-holding, and difficulty swallowing because of uncontrollable oral secretions. Considering this clinical presentation and the historical context of early rabies treatment attempts, which of the following histologic findings in the brain would be most likely present in a rabid animal?
Practice by Chapter
Cellular Pathology of the Nervous System
Practice Questions
Cerebrovascular Diseases
Practice Questions
Trauma to the Central Nervous System
Practice Questions
Infections of the Nervous System
Practice Questions
Demyelinating Diseases
Practice Questions
Neurodegenerative Diseases
Practice Questions
CNS Tumors
Practice Questions
Peripheral Nerve Disorders
Practice Questions
Neuromuscular Junction Diseases
Practice Questions
Congenital and Developmental Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app