
Neuropathology — MCQs

On this page
Multiple cystic lesions are seen in the muscle and brain of a 16-year-old boy who died of status epilepticus. What is the most likely diagnosis?
Aggregates of 'tau protein' seen in the Hippocampus of an elderly man are indicative of which of the following?
Which of the following tumors is associated with drop metastasis?
Which of the following statements about metastases of malignant tumors of the brain is TRUE?
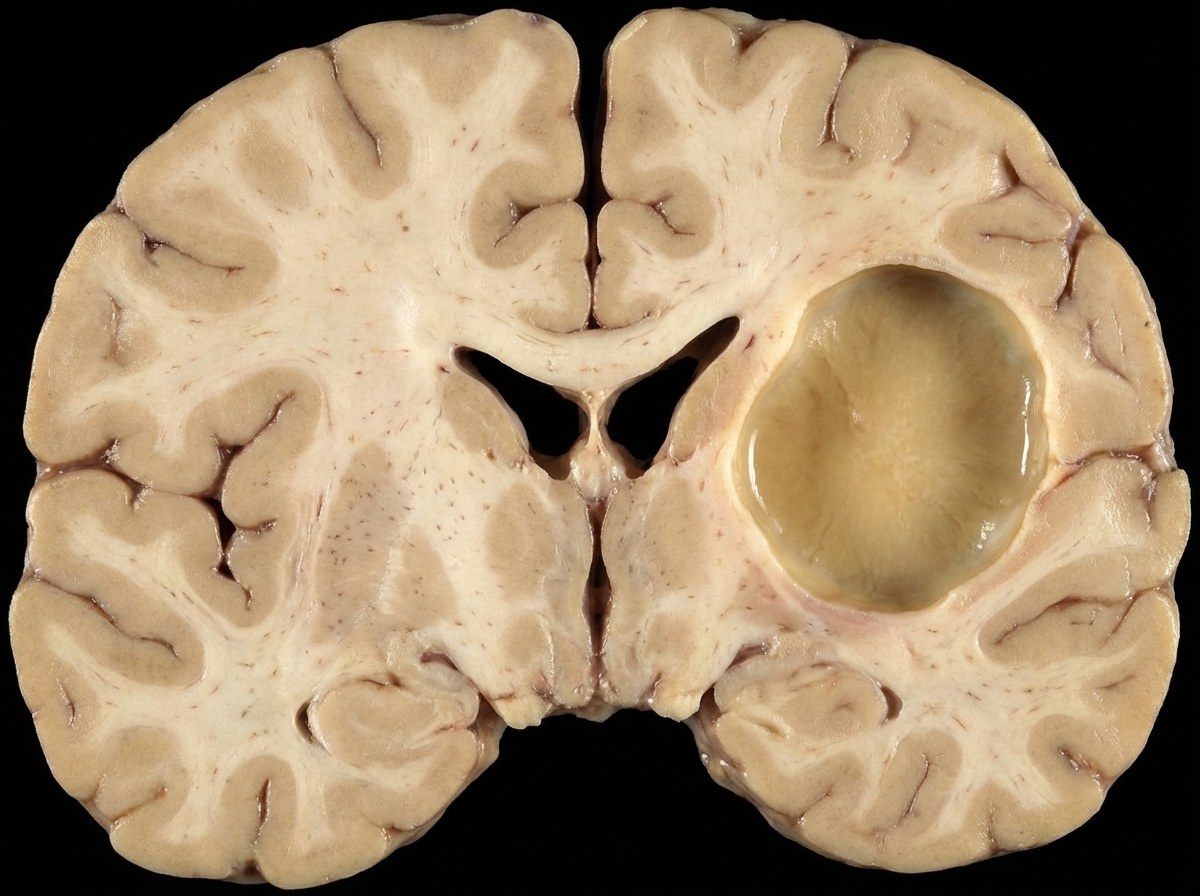
The given lesion is best associated with which of the following conditions?
Wilsons disease primarily affects which part of the CNS?
What is the pathological change observed in the brain in cerebral malaria?
Inclusions in oligodendrocytes are a characteristic feature of which condition?
What genetic mutation leads to Duchenne Muscular Dystrophy?
All of the following are congenital myopathies EXCEPT:
Practice by Chapter
Cellular Pathology of the Nervous System
Practice Questions
Cerebrovascular Diseases
Practice Questions
Trauma to the Central Nervous System
Practice Questions
Infections of the Nervous System
Practice Questions
Demyelinating Diseases
Practice Questions
Neurodegenerative Diseases
Practice Questions
CNS Tumors
Practice Questions
Peripheral Nerve Disorders
Practice Questions
Neuromuscular Junction Diseases
Practice Questions
Congenital and Developmental Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app