
Neuropathology — MCQs

On this page
Which among the following best describes 'Neuropraxia'?
A patient had a road traffic accident (RTA). NCCT head was normal on admission. The patient later died after several days in the ICU due to coma. Brain biopsy revealed multiple punctate hemorrhages. What is the diagnosis?
In Myasthenia gravis, which of the following is the primary target of autoantibodies at the neuromuscular junction?
The CSF findings in bacterial meningitis would include which of the following?
A male presents with a history of vestibular schwannoma and psammoma bodies in the brain. Which of the following is the most likely diagnosis?
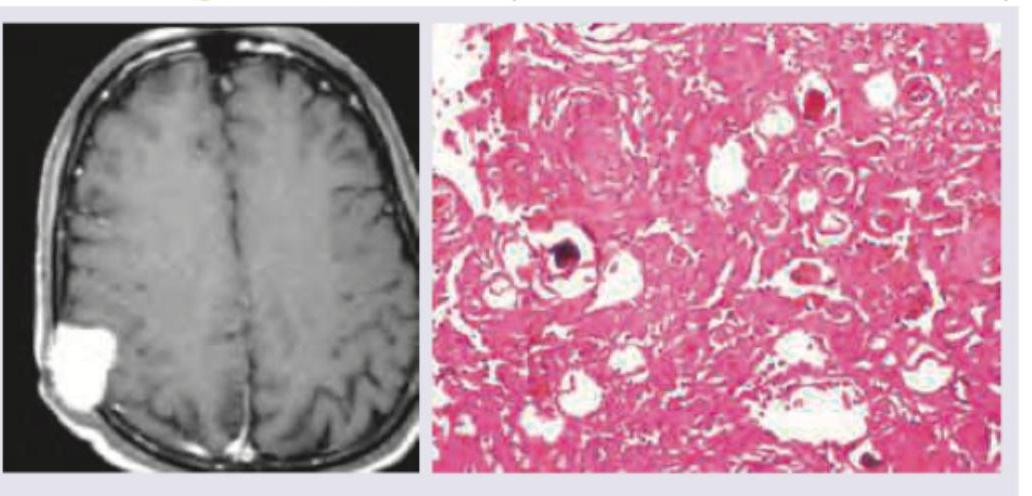
A 40-year-old female presents with frequent headaches. Investigation reveals raised intracranial pressure and the presence of a dural-based tumor. Which of the following histological findings correlate with the diagnosis?
A 25-year old patient who had a Road traffic accident was initially conscious but later became unconscious and subsequently died. On postmortem examination, multiple petechial hemorrhages are seen in the corpus callosum, what is the probable diagnosis?
A 45-year-old female presents with a 2-year history of progressive unilateral hearing loss, tinnitus, and unsteadiness. An MRI scan reveals a well-defined tumor located in the cerebellopontine angle (CPA). A surgical resection is performed, and subsequent histopathological examination of the tumor tissue is given below. Based on these histopathological findings, what is the most likely diagnosis?
A child presents with visual disturbances and delayed growth. Imaging reveals a suprasellar mass, and histopathology shows the presence of "wet keratin" (compact, eosinophilic anucleate keratin). What is the most likely diagnosis?
A 50-year-old woman presents with daily early morning frontal headache and projectile vomiting. The image shows:
Practice by Chapter
Cellular Pathology of the Nervous System
Practice Questions
Cerebrovascular Diseases
Practice Questions
Trauma to the Central Nervous System
Practice Questions
Infections of the Nervous System
Practice Questions
Demyelinating Diseases
Practice Questions
Neurodegenerative Diseases
Practice Questions
CNS Tumors
Practice Questions
Peripheral Nerve Disorders
Practice Questions
Neuromuscular Junction Diseases
Practice Questions
Congenital and Developmental Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app