
Neuropathology — MCQs

On this page
A female is admitted to the ICU with symptoms of Guillain-Barré syndrome (GBS), experiencing these symptoms for the third time within a few weeks. Nerve biopsy reveals an onion-bulb appearance. What is the most probable diagnosis?
A newborn baby has severe facial abnormalities. What could be the underlying central nervous system (CNS) abnormality in this baby?

In chronic alcoholics, what are the acute changes in the brain due to Wernicke's encephalopathy most frequently seen in?
Degenerated neurofilaments seen in patients with Alzheimer's disease are:
What is the most common tumor of the pineal region?
An infant presents with irritability, increased tone of extremities, and recurrent seizures. Tissue examination reveals globoid cells in the parenchyma around blood vessels. What is the most probable diagnosis?
A caseous granuloma is seen in -
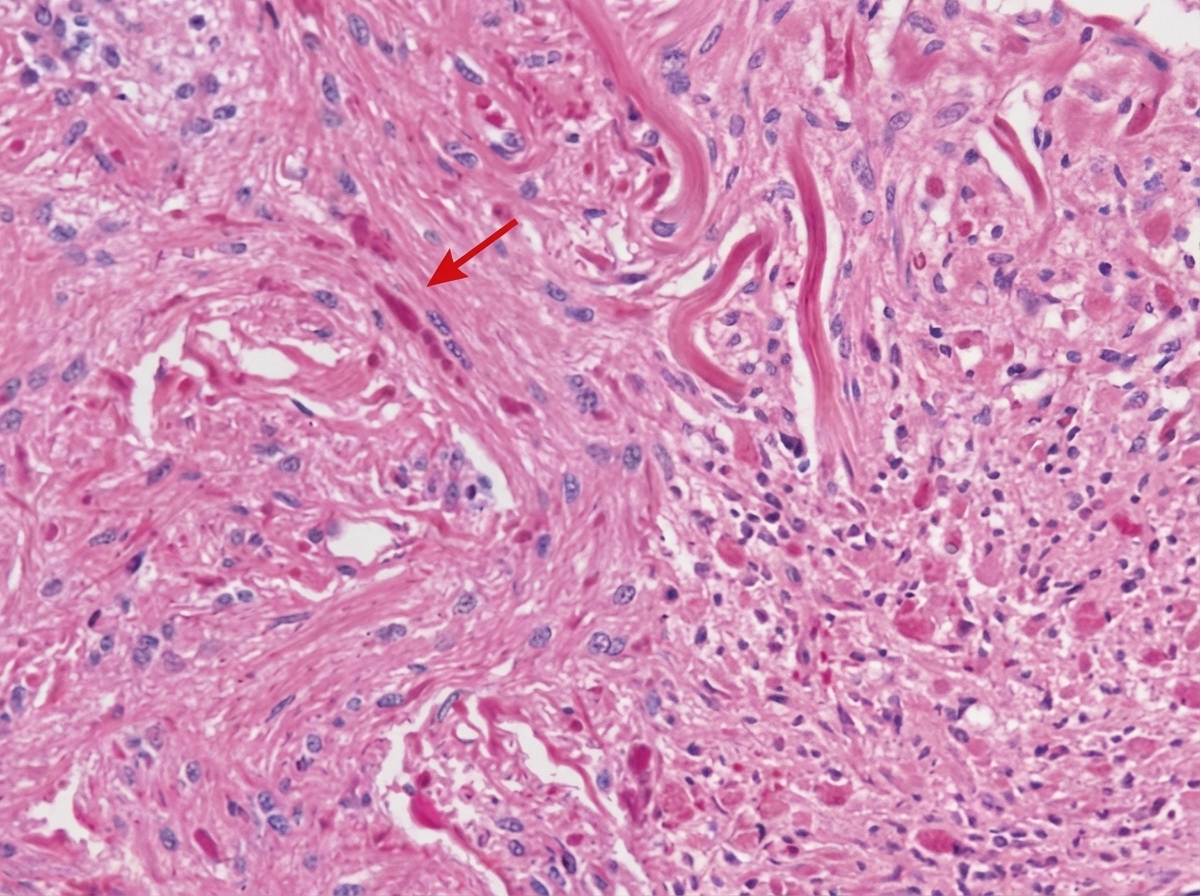
A 10-year-old child presents with a posterior fossa mass. A biopsy reveals dense eosinophilic fibers marked with an arrow. What is the nature of these fibers?
All of the following are true about Duret hemorrhage, EXCEPT:
Which of the following is not seen in CNS involvement in Wilson's disease?
Practice by Chapter
Cellular Pathology of the Nervous System
Practice Questions
Cerebrovascular Diseases
Practice Questions
Trauma to the Central Nervous System
Practice Questions
Infections of the Nervous System
Practice Questions
Demyelinating Diseases
Practice Questions
Neurodegenerative Diseases
Practice Questions
CNS Tumors
Practice Questions
Peripheral Nerve Disorders
Practice Questions
Neuromuscular Junction Diseases
Practice Questions
Congenital and Developmental Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app