
Neuropathology — MCQs

On this page
Which is the most common intracranial brain tumor in adults?
Which of the following sites in the brain is a common location for ischemic damage, rabies virus infestation, and toxic damage resulting from alcohol?
A 54-year-old male presents with gradual onset of mild dementia, ataxic gait, and myoclonus. An MRI scan is normal, and cerebrospinal fluid analysis reveals no abnormalities. However, the patient's EEG is remarkable for recurrent bursts of high-voltage slow waves. Over the next 6 months, the patient's dementia rapidly worsens, accompanied by hypertonicity and profound dysarthria. The patient dies shortly thereafter. Which of the following is the most likely neuropathological finding on autopsy?
A 65-year-old woman with a history of breast cancer and a recent melanoma presents to the emergency room following a tonic-clonic seizure. Blood chemistry values are within normal limits. There is no history of drug or alcohol use. MRI of the brain shows bilateral cerebral edema and a cystic, frontal lobe lesion. Frozen section obtained from a CT-guided biopsy reveals a hemorrhagic nodule of neoplastic cells. Immunohistochemical stains for which of the following antigens would be most helpful in making your diagnosis definitive for melanoma?
Regarding Progressive multifocal leucoencephalopathy, all are true, except?
Which of the following statements is true about medulloblastoma?
All of the following are true about Primary CNS Lymphoma except:
What is the most common central nervous system (CNS) manifestation of HIV infection?
A 10-year-old boy presents with persistent headaches for 3 months. He has an ataxic gait and dysdiadochokinesia. A CT scan reveals a 4-cm cystic mass in the right cerebellar hemisphere with enlarged lateral ventricles. CSF analysis shows elevated protein and normal glucose. Intraoperative gross examination of the resected mass shows a cyst filled with gelatinous material, a thin wall, and a 1-cm mural nodule. Microscopic examination reveals cells positive for glial fibrillary acidic protein (GFAP) with long, hair-like processes. What is the most likely diagnosis?
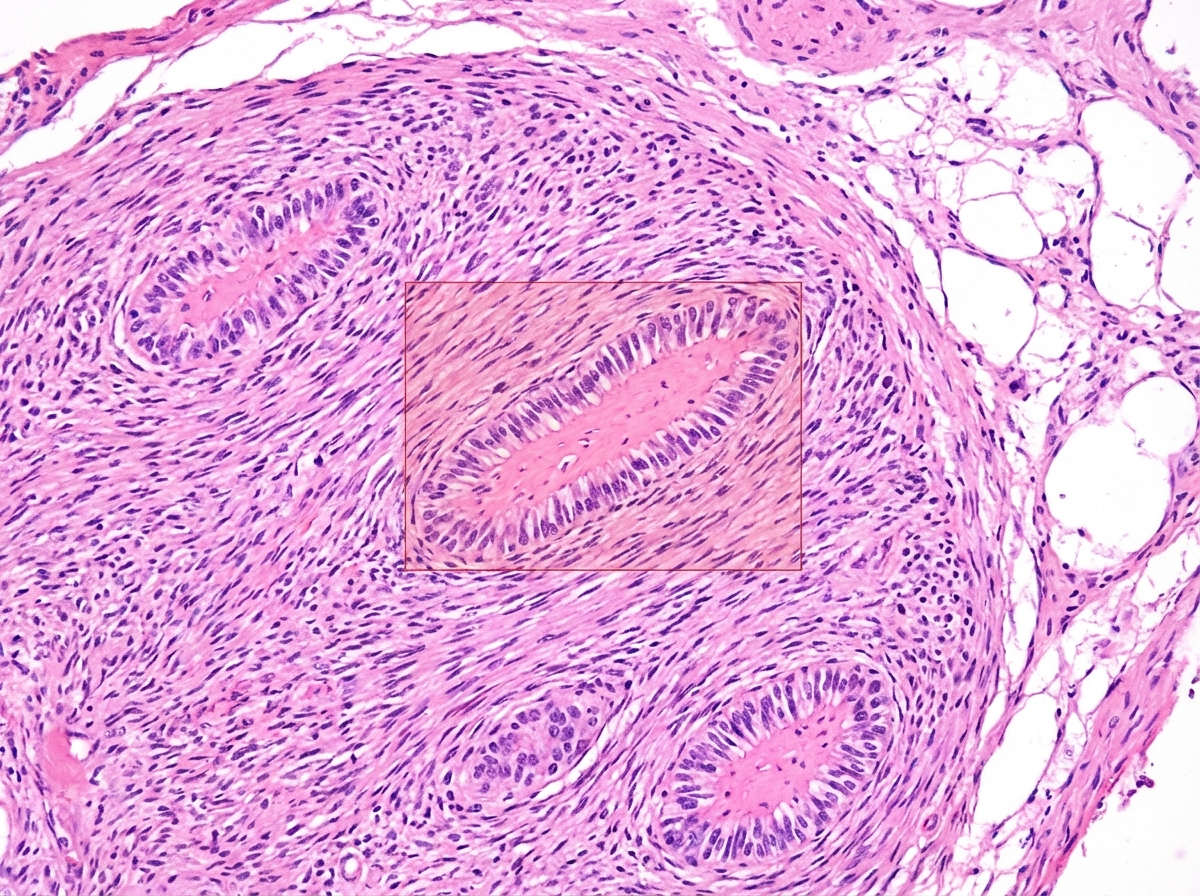
The marked area in the image of a Schwannoma represents which of the following?
Practice by Chapter
Cellular Pathology of the Nervous System
Practice Questions
Cerebrovascular Diseases
Practice Questions
Trauma to the Central Nervous System
Practice Questions
Infections of the Nervous System
Practice Questions
Demyelinating Diseases
Practice Questions
Neurodegenerative Diseases
Practice Questions
CNS Tumors
Practice Questions
Peripheral Nerve Disorders
Practice Questions
Neuromuscular Junction Diseases
Practice Questions
Congenital and Developmental Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app