
Neuropathology — MCQs

On this page
A 45-year-old man presents with weakness and wasting of the muscles of his right hand for 8 months. Physical examination shows fasciculations of the hand. The patient's speech is impaired, and 6 years later, he dies of respiratory insufficiency. Autopsy shows atrophy of ventral roots in the spinal cord. Which of the following is the most likely diagnosis?
In Tuberous sclerosis, which of the following is NOT typically seen?
Peripheral nerve sheath tumors include all of the following except:
Spongiform changes in astrocytic tumor with neuronal loss is seen in?
A 50-year-old man presents with a staggering gait and lightning pain in his hands and legs. His past medical history is significant for an aortic aneurysm and aortic insufficiency. Neurologic examination reveals impaired senses of vibration, as well as touch and pain in the lower extremities. The patient subsequently dies of pneumonia. Autopsy discloses obliterative endarteritis of meningeal blood vessels and atrophy of the posterior columns of the spinal cord. What is the appropriate diagnosis?
Which of the following gene is associated with Alzheimer's disease?
A neuropathologist is performing an autopsy on a 65-year-old man who had resting tremor, rigidity, and akinesia. Histologic sections of the substantia nigra reveal neurons containing round eosinophilic inclusions. Such inclusions most likely represent?
Genetic alteration in which of the following chromosomes can lead to oligodendroglioma?
A 50-year-old woman presents with a 5-year history of headaches, generalized tonic-clonic seizures, and bilateral leg weakness. Skull films reveal hyperostosis of the calvarium. Biopsy of the responsible lesion shows a whorling pattern of the cells. Which of the following is the most likely diagnosis?
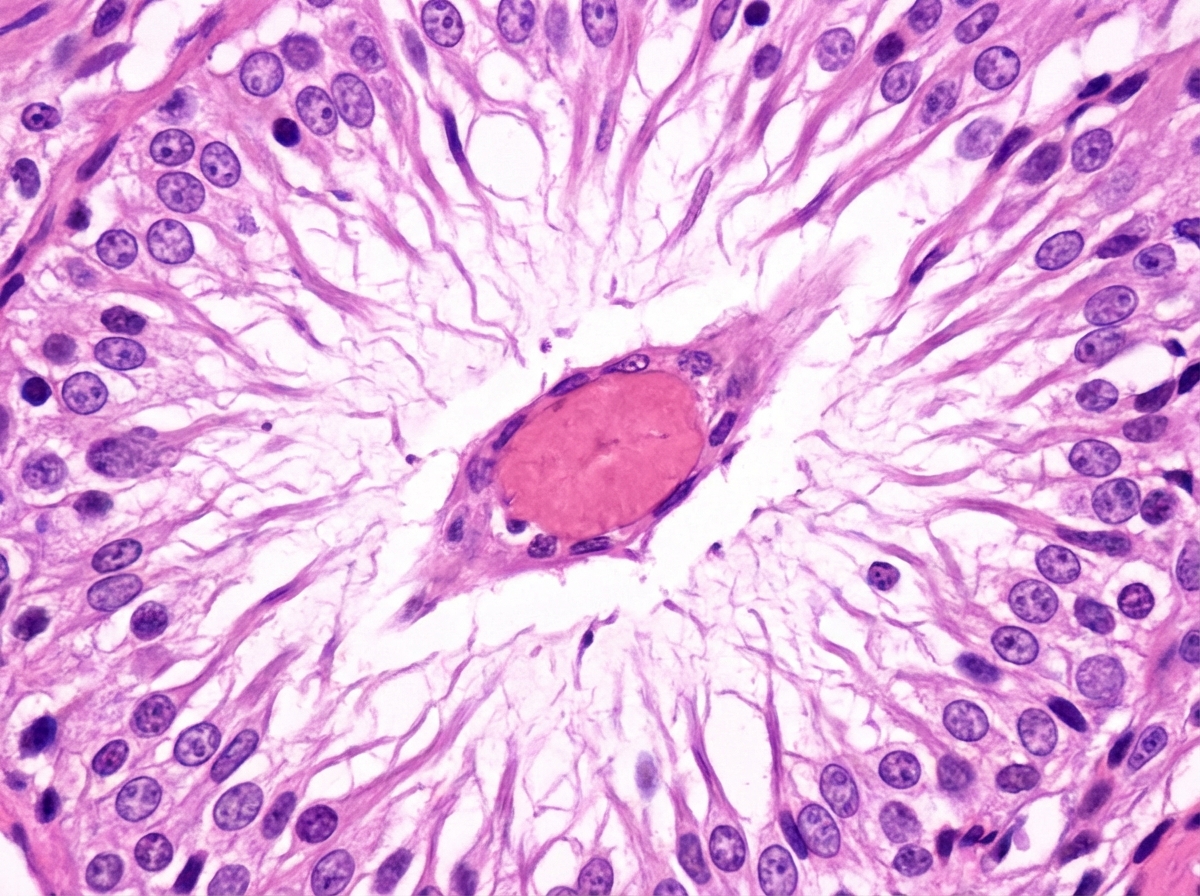
Identify the rosette shown.
Practice by Chapter
Cellular Pathology of the Nervous System
Practice Questions
Cerebrovascular Diseases
Practice Questions
Trauma to the Central Nervous System
Practice Questions
Infections of the Nervous System
Practice Questions
Demyelinating Diseases
Practice Questions
Neurodegenerative Diseases
Practice Questions
CNS Tumors
Practice Questions
Peripheral Nerve Disorders
Practice Questions
Neuromuscular Junction Diseases
Practice Questions
Congenital and Developmental Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app