
Parasitology — MCQs

On this page
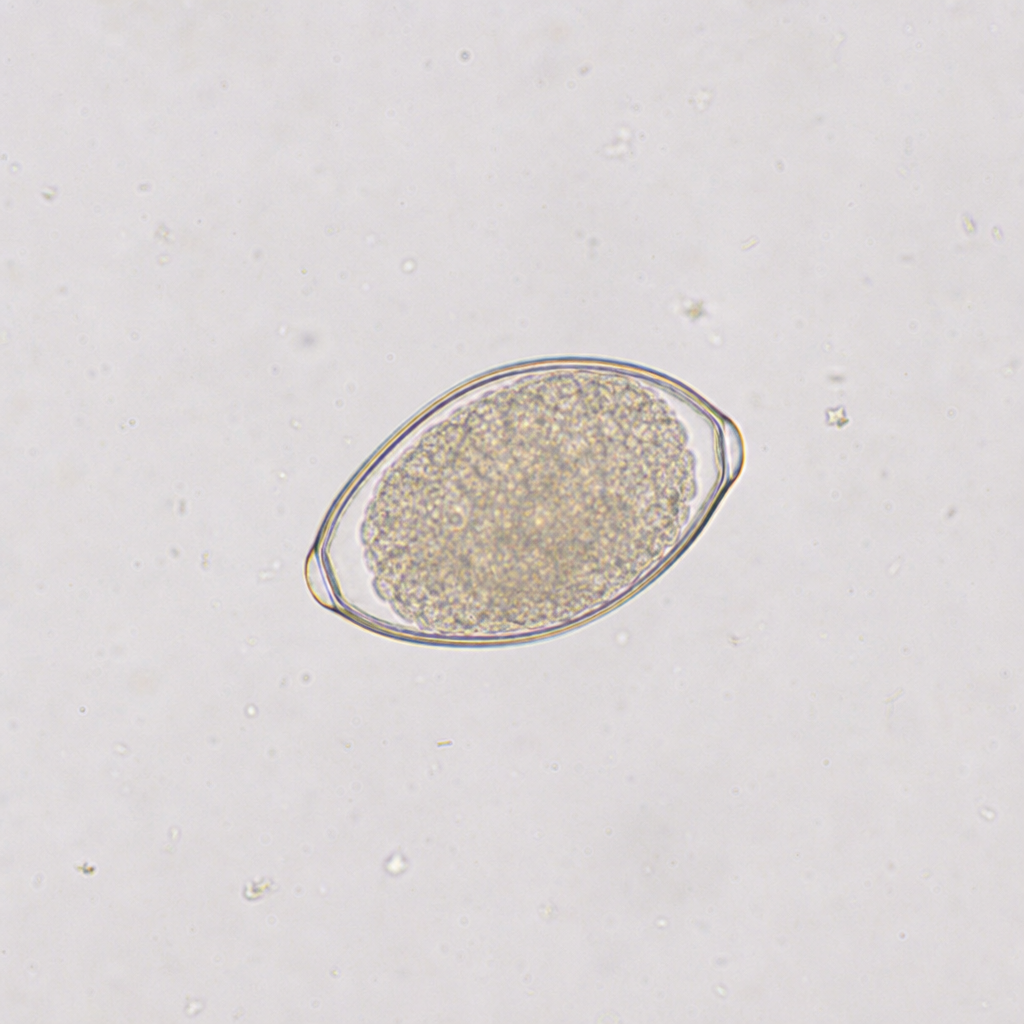
An 8-year-old child presents with perianal itching. Perianal scraping/swab shows the following bile non-stained eggs. What is the causative parasite?
All of the following are true of Neurocysticercosis EXCEPT?
Why are schizont and late trophozoite stages of Plasmodium falciparum not observed in peripheral blood smears?
An HIV patient presented with diarrhea. Stool examination revealed acid-fast organisms. What is the drug of choice for this patient?
What is the primary reservoir for hookworm infection?
Which parasite is characterized by a cyst containing a scolex with hooks?
A patient presents with features of biliary obstruction and a history of consuming raw fish during a recent trip. Which of the following is the most probable etiology?
Infection with which organism during pregnancy can cause congenital hydrocephalus?
Which of the following parasitic infections predisposes to malignancies?
Which of the following statements about Entamoeba histolytica is incorrect?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app